
Como todos los años, El Centro de estudios en cardiología intervencionista realizo su Simposio Anual, se llevó cabo en el auditorio del Sanatorio Otamendi el día 18 de Noviembre de 17 a 21:30hs.
podrá verlo en este link

Programa CECI 2022
Módulo Estructural 17:05 a 18:30
Moderadores Dr Carlos Fernandez-Pereira, Dr Ricardo Perez de la Hoz.
17:05-17:20 Estado actual de la evidencia de TAVI en estenosis aórtica con riesgo bajo e intermedio.
Dr. Ron Waksman.
17:20-17:30 La relación con la alteración de la conducción AV durante y después del TAVI
Dr. Héctor Vetulli
17:30-17:40 Angioplastia coronaria y TAVI: antes, durante o posterior
Dr.Juan Mieres
17:40-17:55 Casos enlatados de TAVI Vita Flow.
Dr.Carlos Fernandez-Pereira, Hernán Pavlovsky, Dr.Diego Ascarrunz
17:55-18:05 Single,double or triple DAPT post TAVI
Dr. Matías Rodriguez Granillo
18:05-18:20 TAVI en válvula aórtica bicúspide e insuficiencia aórtica: Evidencia clínica.
Dr.Ron Waksman
18:20-18:30 Panel de Discusión. Dr.Eduardo Carrasco ,Dr Hernan Pavlovsky, Dr Camila Gallardo, Dr Federico Vigo, Dra Lucia Fontana.
18:30-18:45 Break
Módulo SCA 18:45 a 20
Moderador: Dr Dario Vita – Dr Matías Rodriguez Granillo
18:45-19:00 DAPT en pacientes con alto riesgo de sangrado
Dr Peter Smits.
19:00-19:15 Evidencia clínica de prasugrel/ticagrelor en pacientes post PCI
Dr Adnan Kastrati.
19:15-19:25 Evidencia clínica de DAPT en pacientes con STEMI y alto riesgo de sangrado
Dr Peter Smits.
19:25-19:35 ¿Clopidogrel debería ser la nueva aspirina en el mantenimiento de la terapia, luego de un SCA?.
Dr Ernesto Duronto.
19:35-19:45 IAM con Múltiples Vasos: La Revascularización «más completa» incluye a la Prevención Secundaria.
Dr Gustavo Samaja.
19:45-20:00 Panel de Discusión :
Dra Bibiana Rubilar- Dr Gaston Procopio- Dra Sandra Swieszkowski, Consejo de
Cardiología Clínica.
Módulo Enfermedad Coronaria 20:00 a 21:30
Moderador: Dra Valeria Curotto – Dra Carolina Salvatori.
20:00-20:10 Rol de las imágenes cardiovasculares, RMN y TMC, en la estratificación de los pacientes coronarios.
Dr. Fernando Dettori
20:10-20:20 Revascularización en pacientes con FEVI deteriorada; estado de la evidencia actual
Dr Jorge Thierer.
20:20-20:30 Porque debemos hacer angioplastia en pacientes crónicos y con deterioro de la función ventricular izquierda después del ISCHEMIA y REVIVED?
Dr Alfredo Rodriguez .
20:30-20:45 Ventajas de la combinación de drogas en los stents liberadores de fármacos para prevención de eventos adversos en población general y en diabéticos
Dr Adnan Kastrati .
20:45-20:55 Podemos usar corta DAPT en pacientes de complejidad media o alta?
Dr Peter Smits
20:55-21:10 Presentación de Casos clínicos.
Dra Giuliana Tresenza
21:10- 21:30 Panel de Discusión.Dr Miguel Rubio,Dr Ruben Piraino, Dr Camila Correa,Dr Carlos Rodriguez Pagani ,Dr Miguel Rosales.
Break y Cena.
Read MoreAlfredo E Rodriguez MD ,PhD, FACC,FSCAI
Debo agradecer la excelente oportunidad que nos brinda el Colegio Argentino de Cardioangiologos Intervencionistas (CACI) a los que fuimos miembros fundadores del Colegio y practicamos la especialidad hace ya más de 40 años.
A través de estas páginas tratare de resumir lo que considero los elementos más importantes vividos por todos nosotros desde el inicio de la especialidad y que además estuvo muy ligado a lo que sucedió y sucede en el mundo con esta fascinante y cambiante especialidad. En el año 1980, estando como jefe de Residentes del servicio de Cardiología/Hemodinamia/Cirugía Cardiovascular del Sanatorio Guemes entonces Fundación Favaloro, cuyos Directores eran los Drs Rene G. Favaloro y Luis de la Fuente, comenzamos hacer nuestras primeras armas en angioplastia periférica, de arterias femorales y también de arterias renales, no teniendo todavía la capacidad operativa y técnica para comenzar este tratamiento en arterias coronarias.
Tres años antes habían dejado el servicio quienes fueron lideres de ese momento los Drs Marcelo Ruda Vega y Hugo Londero y estaban como staff los Drs Jorge Leguizamón y Eduardo Picabea
En ese entonces hacia casi tres años que el Dr Andreas Gruntzig presentaba sus primeros casos realizados en Zúrich en 1977 en un meeting del American Heart Association.
También por ese entonces, en 1979 Peter Rentrop mostraba los beneficios de la trombólisis intracoronaria con estreptoquinasa para reperfundir pacientes en las primeras horas de un infarto agudo de miocardio.
La cardiología intervencionista comenzaba a nacer.
Es justamente en el año 1980, precisamente el día 3 de octubre, día de mi cumpleaños, que tuve la oportunidad de realizar mi primera experiencia en terapéutica por catéter en cardiopatía isquémica en un paciente con infarto agudo supra ST.
El paciente tenía 12 horas de un post operatorio de bypass venoso “side to side” a las arterias Descendente Anterior y Diagonal que presentaba un infarto extenso anterolateral con compromiso hemodinámico.
El Dr Favaloro llama a Hemodinamia, hablo con él y le propongo la posibilidad de infundir trombolíticos en el sitio de la posible oclusión es decir el bypass Aorto coronario con vena safena.
El conocido hematólogo Raúl Altman, trabajaba asociado estrechamente con el Dr Favaloro y además contaba con Uroquinasa para tratamientos específicos.
Con estos elementos cateterizamos selectivamente el bypass ocluido y le infundí Uroquinasa in situ durante una hora lográndose la reperfusión de la arteria Diagonal y todo el tercio proximal y medio de la Descendente Anterior con flujo TIMI 3 y completa estabilización hemodinamica.
Recuerdo con mucha alegría que el Dr Favaloro me llamo y me dijo: “Rodriguez este es tu mejor regalo de cumpleaños”
Este caso lo presente en un congreso Sudamericano de Cardiología y dos años después se publicó junto con otro caso realizado posteriormente por otro staff del servicio de Hemodinamia en la revista del American Heart Association como Case Report.
Increíble que a pesar de haberlo realizado yo personalmente como se dice en la jerga quirúrgica “ de piel a piel” fui excluido deliberadamente de la publicación sin mi conocimiento y aprovechando mi ausencia debido a numerosos viajes realizados a USA durante los años 1981/82.
En ese año 1980 el Dr Richard Myler pionero de angioplastia en USA da conferencias en el Sanatorio Güemes invitado por el Dr Favaloro.
Ahí surge la posibilidad de viajar a su Servicio, cosa que lo hice en Enero de 1981 estadia que se prolongó por tres meses. Anos mas tarde, fue el Dr Myler que me presento y posibilito mi acceso como Fellow del American College of Cardiology.
En ese lapso, también tuve la oportunidad de visitar al Dr John Simpson en la Universidad de Stanford que estrenaba un nuevo sistema de catéteres y guías metálicas móviles para angioplastia coronaria, sistema que se denominó “steerable”.
En abril estando ya en Argentina, comenzamos a realizar las primeras angioplastias coronarias en el Sanatorio Guemes.
La angioplastia en Europa y USA estaba en plena ebullición, con varios pioneros además de Gruntzig en Suiza, uno de los mas importantes el Dr Geofrey Hartzler en Kansas, USA, sin duda el nombre más importante en angioplastia en infarto agudo de miocardio que falleció lamentablemente en forma muy temprana.
Hartzler en 1982 introduce el método de hacer angioplastia primaria sin trombólisis previa lo que se llama angioplastia directa.
La angioplastia en infarto agudo de miocardio era por entonces muy controversial, con resultados contradictorios y la mayoría se hacía después de la infusión de trombolíticos.
A fines de 1981 un año después de haber realizado la trombólisis intracoronaria antes descripta, tuve la oportunidad de efectuar una angioplastia post trombólisis en un paciente con infarto agudo supra ST de pared inferior por oclusión de la arteria Coronaria Derecha, primero reperfundí la misma con infusión intracoronaria de Uroquinasa y luego se practicó angioplastia por balón exitosa.
Este caso fue publicado a principios del año 1982 en la Revista de la SAC (1) a mi conocimiento fue el primer caso de angioplastia coronaria post trombólisis en el infarto agudo de miocardio realizada en América Latina y probablemente solo un grupo alemán fue contemporáneo que en ese mismo año 1982 publicaron dos casos en la revista Circulation.
En toda esta década de 1980 se produce el boom de nuestra especialidad en todo el mundo occidental, tanto USA como Europa muestran la explosión de nuestra especialidad, la angioplastia coronaria con balón (POBA) es también a fines del 80 acompañada con otros “devices” como aterotomo direccional, rota ablación, balón de dilatación e infusión prolongada etc hacen su aparición y nos permiten realizar angioplastias mas complejas que las inicialmente seleccionada por Gruentzig.
Es en esos momentos, mediados de la década del 80 que iniciamos nuestro propio grupo de trabajo clínico en 1986 pero también de investigación clínica el Centro de Estudios en Cardiología Intervencionista (CECI) que persiste hasta el presente.
En esos momentos comenzaban a surgir con fuerza experiencias limitadas pero muy prometedoras en el uso del stent metálico (BMS) para prevenir las oclusiones coronarias durante la angioplastia con balón, y los nombres de Sigwart, Puel, Marco, Serruys, Roubin y de Palmaz comienzan a escucharse muy frecuentemente en todos los ámbitos científicos de nuestra especialidad.
# Décadas 1990/2000/2010 o el ascenso vertiginoso de la angioplastia como método terapéutico del paciente coronario agudo y crónico.
Estas fueron en mi opinión las décadas “doradas” de nuestra especialidad.
La primera 1990/2000 mostro la consolidación del uso del stent metálico durante las angioplastias para tratar las complicaciones agudas como así también la reestenosis coronaria post POBA evitando el “recoil agudo y crónico” post angioplastia con balón que era por entonces la causa principal de reestenosis post balón. El uso del BMS lo introducen en USA los Drs Roubin y Palmaz con sus dispositivos balón expandible, el primer BMS aprobado por la FDA en USA para tratar complicaciones agudas fue el de Gianturco-Roubin seguido poco tiempo después por el Palmaz-Schatz.
El uso del stent se introduce en todas las condiciones clínicas inclusive el infarto agudo de miocardio y en lesiones coronarias muy complejas.
En esta década,1990/2000, se publican los primeros estudios aleatorizados de angioplastia coronaria con POBA versus cirugía coronaria directa (CABG) en pacientes con obstrucciones simples, de múltiples vasos, mayoritariamente con enfermedad coronaria crónica y en pacientes diabéticos . Posteriormente, estas mismas comparaciones se harían con el uso de BMS. También es la época de los estudios aleatorizados comparativos en el infarto agudo de miocardio entre angioplastia versus trombólisis y luego angioplastia con POBA versus angioplastia con stent .
En la década siguiente ,2000/2010, dos importantes metaanálisis demostraron que a largo plazo la angioplastia en pacientes con enfermedad multi vaso tiene la misma sobrevida y sobrevida libre de infarto comparativamente a la CABG excluyendo los pacientes diabéticos. En estos análisis la sobrevida en pacientes jóvenes mostraba una clara ventaja a favor de la angioplastia, hecho entendible pero que se demostró por primera vez en este metaanálisis . La única diferencia a favor del CABG eran la mayor frecuencia de nuevos requerimientos de revascularización con angioplastia.
Lamentablemente, estos hallazgos se publicaron,2008/2009, en el preciso momento del auge de los DES, por lo tanto, estos resultados fueron pasados por alto.
El uso del BMS si bien había minimizado las complicaciones agudas de la angioplastia su uso producía una reestenosis del mismo por hiperplasia fibrointimal producto de una cicatrización exagerada que producía nuevas reintervenciones del vaso tratado durante los primeros 8-10 meses post implante en un 15% /20% .
La introducción de drogas inmunosupresoras en el stent que se liberaban durante el primer mes post implante en el endotelio arterial producía una reducción significativa de esa hiperplasia y una importante reducción de nuevas revascularizaciones. Con esta combinación evitábamos tanto el recoil agudo como también la hiperplasia fibrointimal.
Esto es el inicio de los stents liberadores de fármacos (DES) que revolucionaron y aun hoy en algunos foros de discusión, no en el mío propio, siguen revolucionando nuestra especialidad. Los nombres de Antonio Colombo, Eberhard Grube, Martin Leon, Patrick W. Serruys y Greg Stone es en gran medida, a ellos a quien se les debe este salto tecnológico con la introducción de los stents liberadores de fármacos (DES). En este punto, nuestro colega Eduardo Sousa y su grupo en Brasil jugaron también un rol relevante. Sin embargo, nuestro país nuevamente no estuvo ausente en este desarrollo de los DES, y uno de los estudios observacionales en su uso fue realizado en Argentina por el Dr Luis de la Fuente y a pesar de que sus hallazgos no fueron refrendados por un largo estudio multinacional aleatorizado europeo, que se debió finalizar prematuramente por exceso de complicaciones trombóticas de este diseño de DES, este estudio piloto fue pionero en ese momento.
En los últimos 15 años son múltiples los grupos de investigadores argentinos que participaron en estudios con el uso de DES.
La reducción significativa de nuevas revascularizaciones post DES nos hicieron abrir expectativas demasiado optimistas con el uso de este: “el fin de la reestenosis era el fin también de la CABG” según se escuchaba con el resultado de los primeros estudios aleatorizados con DES. En el apartado siguiente veremos cuán lejos estamos hoy de esas predicciones.
Este exceso de optimismo en realidad estaba basado en reducción de puntos finales completamente secundarios y no clínicos como la reducción del llamado “late loss” que nunca pudo ser correlacionado con eventos duros post angioplastia.
.
# Década 2010/2021 Del ascenso vertiginoso como indicación de revascularización hasta la realidad actual.
En este punto voy a ser muy directo, pero también muy crítico y mis opiniones deben tomarse también desde el punto de vista personal.
Con el advenimiento del uso DES en la práctica clínica, múltiples trabajos aleatorizados comparativos entre la angioplastia con DES versus la CABG se han realizado a la fecha, hasta el presente podemos contabilizar 8 estudios tres en lesiones de tronco no protegido, uno en múltiples vasos y tronco y los cuatro restantes en múltiples vasos incluyendo pacientes diabéticos.
Todos excepto uno, invariablemente mostraron aumento no solo de los procedimientos de revascularización que fue un acompañante natural de la angioplastia desde su inicio y que no debería preocuparnos, sino que también en 7 de ellos se observó un incremento de mortalidad y/o infarto espontaneo de miocardio que es el más preocupante y que se asocia a mortalidad.
La mayor complejidad de los pacientes tratados podría ser una de las explicaciones de estos hallazgos, pero seguramente no la única de hecho diversos metaanálisis han demostrado que independientemente de la complejidad anatómica la CABG tuvo menor incidencia de eventos duros como infarto de miocardio y en algunos estudios también de mortalidad.
Este cambio en los parámetros de seguridad en estudios comparativos con cirugía ya se había observado en el largo registro americano del ASCERT con 190 mil pacientes tratados con CABG y PCI (78% DES1) durante los años 2004 a 2008 en 64 sitios de USA y donde en pacientes >64 años hubo significativa reducción de la mortalidad con CABG incluso en grupos de riesgo angiográfico y clínico bajo (no diabéticos y lesión de dos vasos) y que motivo que nosotros escribiésemos un artículo de revisión en el año 2012, donde ya llamábamos la atención sobre estos hallazgos. Esta referencia esta dentro de los artículos sugeridos para leer.
Si bien es totalmente cierto que los DES redujeron notablemente la incidencia de nuevas revascularizaciones la mortalidad no se modificó cuando comparamos con los viejos diseños de DES y/o incluso los BMS.
El uso de DES tuvo con los primeros diseños cuatro limitaciones algunas de ellas entrelazadas:
1-Stent trombosis precoz, tardía y muy tardía.
2-Mala aposición tardía del DES. Estas dos eran muchas veces correlativas
3- Neo-aterosclerosis precoz inmediatamente después del ano del implante.
4- Disfunción endotelial tanto en el stent como en los segmentos proximales y distales al implante.
Stent trombosis y mala aposición dependían fundamentalmente del polímero y hoy podemos decir que es un tema completamente solucionado.
Sin embargo, las dos restantes neo-aterosclerosis precoz y disfunción endotelial dependería principalmente de la acción local de la droga inmunosupresora. La primera es causa de infarto espontaneo no relacionado a un nuevo procedimiento fenómeno que estamos observando casi invariablemente en todos los estudios aleatorizados comparativos con la CABG. La disfunción endotelial también esta asociado a efectos adversos cardiacos, pero últimamente también con efectos adversos no cardiacos incluyendo aumento de frecuencia de tumores sólidos. No hay que olvidarse que el endotelio es un órgano con múltiples funciones como: “vasodilation, thrombolysis, platelet disagreggation, antioxidant, antiinflammation, antiproliferation”.La pérdida de su función normal es decir la disfunción endotelial podría producir los efectos contrarios: “vasocontriction, thrombosis, platelet agreggation, oxidant activity, inflammation and growth factors”. En este punto es muy importante que los cardiólogos intervencionistas definamos costo/beneficio entre supresión de restenosis / disfunción endotelial y las consecuencias de esta última.
Sobre este tema recomiendo leer los manuscritos referenciados abajo por Toya y col y Abdul-Jawad Altisent y col, dentro de las ultimas referencias de este capítulo.
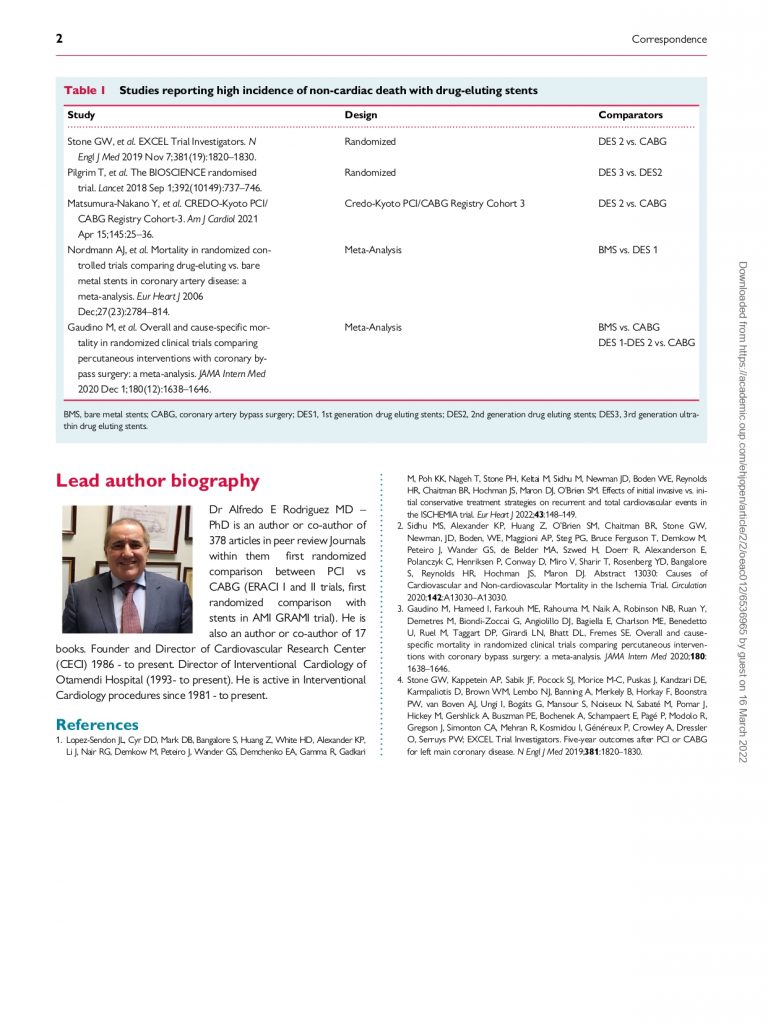
Llama la atención varias observaciones relacionadas con mortalidad no cardiaca en pacientes tratados con angioplastia en el momento actual que no estaban presentes en observaciones previas y esto debería ser motivo de cuidadoso análisis en estudios aleatorizados apropiadamente realizados, así como en registros prospectivos. Este aumento de mortalidad no cardiaca se observó en estudios aleatorizados entre DES y CABG, pero no entre BMS y CABG, en registros de PCI y CABG muy conocidos y también entre comparaciones de diferentes diseños de DES. Recomiendo leer el metaanálisis de Gaudino, los 5 años del EXCEL, el estudio de Pilgrim a 5 años de un”ultrathin DES”, el registro CREDO-Kyoto de angioplastias y CABG todos referenciados abajo así como también el abstract del ISCHEMIA trial publicado en Circulation en Noviembre del año pasado y del European Heart Journal este ano. La publicación de este ultimo motivo un comentario Editorial nuestro que esta publicado en el European Heart Journal Open en Febrero de este ano y en donde en una Tabla describimos todos los estudios que reportaron aumento de muerte no-cardiaca con DES en seguimiento a largo plazo, a estos deberemos incluir los hallazgos del estudio ISCHEMIA que es realmente muy preocupante.
Como sabemos los estudios randomizados con tamaño suficiente tienen el poder de homogenizar basalmente las poblaciones por lo cual la explicación del aumento de eventos adversos inesperados en poblaciones aleatorizadas grandes deberá buscarse en otros escenarios.
Denominar a hallazgos adversos, muerte no cardiaca, como fruto de la casualidad me parece una actitud temeraria y fuera de toda lógica que obviamente le hace mucho daño a nuestra especialidad.
Solo una sincera discusión de todos estos hallazgos entre los lideres de opinión juntamente con la Industria podremos salir de este laberinto que nos encontramos ahora donde cada nuevo estudio aleatorizado tanto con CABG o con tratamiento médico nos lleva una nueva frustración.
Últimamente inclusive la introducción de métodos de diagnóstico funcional de lesiones coronarias como el FFR o iFR para guiar la PCI no han sido exitosos en demostrar reducción de eventos post implante de DES tanto en pacientes con infarto agudo o pacientes electivos, recomiendo leer los resultados publicados este ano de estudios randomizados al respecto entre ellos el FUTURE, FAME 3 y el de Puymirat E et al en infarto agudo de miocardio todos referenciados abajo entre las lecturas sugeridas. Los resultados negativos de estos estudios con FFR nos demuestran que rápido los cardiólogos intervencionistas adoptamos técnicas y nuevos “devices” generando muchas veces falsas expectativas por una sobreestimación apresurada de los beneficios.
Las nuevas guías de tratamiento recientemente elaboradas en conjunto con cardiólogos clínicos que en mi criterio fueron benévolas con nosotros, muestra que contrario a lo que se pregonaba 15 años atrás y a pesar del advenimiento de los más modernos diseños de DES, la cirugía coronaria esta más viva que nunca. De hecho, las Sociedades Americanas (USA) y Europea de Cirugía Torácica y Cardiovascular no endorsaron dichas guías de tratamiento.
# Creación del Centro de Estudios en Cardiología Intervencionista (CECI).
En el año 1986 junto con colegas y amigos formamos un grupo de trabajo independiente primero en el Sanatorio Anchorena para luego movernos al Sanatorio Otamendi desde 1993 hasta el presente.
Durante todos estos anos no hay palabras para describir el apoyo a todas nuestras tareas asistenciales y científicas desarrolladas en el Otamendi, vaya pues mi agradecimiento a sus autoridades pasadas los Drs Jose A. De All por quien entre a trabajar en dicha Institución y al Dr Jorge Aufiero así como también a las autoridades actuales.
Durante todos estos años, pasaron por el Servicio a formarse en la práctica de nuestra especialidad muchísimos cardiólogos, muchos de ellos hoy Jefes de Servicio en lugares referentes de nuestro país así como destacados miembros de sociedades científicas que no los podría enumerar por la cantidad, tanto de nuestro país como de América Latina. Por el servicio pasaron residentes de casi todas las nacionalidades de la región de habla española y portuguesa desde Paraguay, Chile, Brasil, Bolivia, Perú, Uruguay, Ecuador, Venezuela, Colombia, Panamá y República Dominicana que luego siguieron conectados con nosotros realizando muchas veces trabajos de investigación en conjunto.
En el año 1988, creamos un departamento de investigación clínica independiente que, si bien no fue concebido como una CRO, donde en Argentina hay varias, algunas de ellas de excelencia, nos permitió realizar en forma ordenada una multiplicidad de protocolos de investigación en nuestro país al principio en forma individual para posteriormente realizar estudios multicéntricos incluyendo multinacionales.
De igual manera realizamos desde 1993 cursos en vivo la mayoría de las veces en forma colaborativa con SAC y CACI los cursos CECI donde han participado como Faculties la casi totalidad de los mayores nombres pasados y presentes de nuestra especialidad de los ultimo 30 años. Este ano, el 7 de Diciembre lo hicimos en forma virtual con la presencia de los Drs Adnan Kastrati, Ron Waksman, Peter Smits y Mario Gaudino.
Vamos a hacer el resumen de los trabajos más importantes y que creo tuvieron un rol en la práctica clínica de nuestra especialidad:
Esto comenzó con lo que fue el primer trabajo aleatorizado publicado entre angioplastia coronaria con POBA versus CABG que fue el estudio ERACI I publicado en JACC en 1993 y 1995. Años después con el advenimiento de los BMS se realizó la segunda versión de este trabajo el ERACI II que a diferencia del primero fue multicéntrico con el acompañamiento de la recordada Liliana Grinfeld en esta oportunidad. El primero y quinto año de seguimiento se publicaron en el JACC en el 2001 y 2005 ambos manuscritos se publicaron simultáneamente con el estudio ARTS de Patrick Serruys.
En el año 1993, publicamos una observación que sugería que la reestenosis post balón era mayormente producida por el “recoil “ agudo de la arteria post dilatación del balón hecho muy novedoso, nunca antes se lo había relacionado. En el modelo animal de restenosis se sabía que el daño endotelial producido por el mecanismo de la angioplastia llevaba a la reestenosis por hiperplasis fibrointimal del vaso meses más tarde, sin embargo, esto no era igual en el ser humano donde la placa aterosclerótica muchas veces es excéntrica y con comportamiento diferentes a la acción del balón de manera que aquellas lesiones que no modificaban su diámetro 24 horas después de la angioplastia con balón la incidencia de reestenosis fue muy baja. Esto fue motivo de varias publicaciones: Am J of Cardiol 1993,1995, Circulation 1995 y en JACC 1998 y tambien de discusiones académicas con lideres de la especialidad que hablaban de: “.. coronary restenosis a time related phenomenom…” por lo cual nuestras observaciones eran totalmente opuestas y fueron motivo de controversias. El tiempo nos dio la razón y Patrick Serruys termino aceptando de que el recoil agudo era un fenómeno muy importante en la fisiopatología de reestenosis post POBA, ahí empezó hablar de “stent like results post POBA” en otras palabras resultados post balón óptimos sin recoil agudo.
Fue muy grato hace 3 años atrás ver en la galería del Congreso del PCR expuesta como uno de los hitos de la angioplastia justamente el trabajo nuestro de stent en elastic recoil OCBAS trial que fue publicado en JACC 1998 conjuntamente con los estudios ERACI I y II.
En el mismo sentido, también fue muy estimulante leer en el libro sobre historia de las intervenciones cardiovasculares y cardiología intervencionista que uno de sus mayores pioneros Gary Roubin cuyo libro mencionado se titulaba “ The First Balloon-Expandable Coronary Stent an Expedition That Changed Cardiovascular Medicine” publicado en el 2015 nos incluyera junto con Julio Palmaz y Rene Favaloro como los únicos latinoamericanos en la lista de los 93 pioneros de Angioplastia e intervenciones cardiovasculares, esta referencia esta también dentro de las lecturas sugeridas.
El uso del stent en el sitio de un infarto agudo de miocardio si bien atractivo era muy polémico, nuestro grupo dado la relación con el querido Gary Roubin publicamos una corta experiencia en el uso de stent en infarto supra ST en Am J of Cardiol 1996, que nos llevó inmediatamente después hacer lo que fue el primer estudio aceptado para su publicación con stent en infarto agudo el GRAMI trial publicado en Am J of Cardiol 1998 que fue contemporáneo al estudio de David Antoniucci de hecho este se publicó dos meses antes en JACC pero el estudio nuestro había sido aceptado dos meses antes que el estudio de Florencia de manera que nosotros cronológica y académicamente estuvimos primero. Anécdotas que siempre nos contamos en las charlas familiares con mi gran amigo de Italia.
Ya entrando en el nuevo milenio, el Centro CECI participo de registros prospectivos y estudios observacionales como los relacionados a DES trombosis publicado en EuroIntervention en Febrero del 2007 ( “Late stent thrombosis the Damocles sword of DES”) un mes antes que el promocionado artículo de Camenzid y Wijns en Circulation, el registro ERACI III, que fue publicado en JACC en 2006 y en el Eur Heart J en 2007 este último trabajo fue motivo de que esta revista europea incrementase su “impact factor” de acuerdo a una carta personal que recibimos del Editor en Jefe de dicha revista.
El artículo de revisión sobre “DES late thrombosis” hubo amigos que me recomendaron no publicarlo porque podría tener reacciones adversa desde la Industria que manufacturaba los DES, a pesar de esos consejos, el trabajo fue enviado y luego de revisión aceptado y publicado en EuroIntervention. Debo decir, además, que nunca sentí reacción adversa de la Industria por esto.
Si los médicos de la carrera de especialidad del CACI se preguntan cómo pudimos desde Argentina realizar tantos estudios que se publicaran en los mayores “Journals” de habla inglesa les diría que todo se logra con trabajo y mucha honestidad en el análisis y observación de los hechos que uno está viendo. Siempre se debe estar seguro de lo que está diciendo y siempre se deberá chequear la información varias veces antes de emitir un juicio más aún si esto implica hallazgos originales fuera de lo establecido y esperado. De hecho, en el momento en que se escribían estos pensamientos, el 30 de Abril de 2022, según Research Gate los manuscritos de datos científicos publicados por nosotros como autores o co-autores merecían 26222 lecturas, 7568 fueron motivos de referencias bibliográficas y tienen 3920 puntos de interés de investigación que son los números más grandes logrados por cualquier grupo o persona individual en nuestro país en el área de cardiología intervencionista.
Las controversias con nuestros hallazgos ocurrieron en varias ocasiones con el “elastic recoil” , los estudios ERACI y con stent en infarto agudo de miocardio. En estos puntos la colaboración con Igor Palacios, Gary Roubin, John Ambrose, William O’Neill y David Antoniucci fueron muy importantes. Como dije en la ocasión de una distinción que me otorgo la Legislatura de CABA: “ los trabajos los hicimos acá en Argentina con ideas totalmente nuestras y pacientes nuestros, pero nada hubiese sido igual si nuestros amigos y colegas de USA y Europa no nos hubiesen apoyado ”.
En el estudio ERACI I, que Favaloro se enojó muchísimo cuando lo hicimos y hablo mal de los hallazgos incluyendo tratar de convencer al cirujano que había operado casi todos los pacientes de que no firmase el manuscrito una vez que estaba aprobado en el JACC, un trabajo argentino publicado en el JACC en el año 1993 tenía pocos precedentes en la cardiología de nuestro país, finalmente primo la racionalidad y el cirujano firmo el trabajo, el Dr Néstor Perez-Balino fue testigo fiel de lo que estoy relatando. Tuve, sin embargo, el gusto de que varios años después, mayo del 2000, cuando ya se había aceptado para su publicación el nuevo ERACI II, Favaloro me llamara por teléfono para felicitarme personalmente por este trabajo y con cálidos recuerdos del pasado compartido en un momento muy difícil de la Fundación y también personal de el a pocos meses antes de su fallecimiento.
En los últimos 20 años Centro CECI participo de varios estudios aleatorizados multinacionales con diversos diseños de DES y diferentes estrategias de revascularización en pacientes con infarto agudo y en pacientes crónicos.
De esta manera participamos en el abciximab en infarto agudo con un stent metálico de carbono, JESTENT trombectomía reolitica en el infarto agudo, FREEDOM, FREEDOM long term outcome DES vs CABG en pacientes diabéticos, MULTISTRATEGY sobre DES y abciximab en infarto agudo , VALENTINES con balón liberador de Paclitaxel, DEFINITION II tratamiento de bifurcaciones con DES incluyendo lesiones de tronco no protegido y últimamente MASTER DAPT comparación de estrategia antiplaquetaria con DES, todos ellos publicados varias veces en NEJM,JAMA,JACC, Circulation, Eur Heart Journal , JACC Intervention y EuroIntervention.
Igualmente, nuestra base de datos fue entregada para su análisis y control de diversos metaanálisis es así que los estudios ERACI y ERACI II se entregaron para la publicación de Pocok en Lancet 1995, Hlatky en Lancet 2009 y JACC 2012, Daemen en Circulation 2008 y Head en Lancet 2018.
De igual manera la base de datos del estudio EUCATAX fue entregada al Dr Valgimigli para su metaanálisis del Lancet 2019 y Circulation 2021.
También, basados en un registro prospectivo de múltiples vasos, es que nació el Score de ERACI como estrategia de revascularización en pacientes con enfermedad de múltiples vasos y tronco de coronaria izquierda, que fue producto mancomunado de varios centros en nuestro país y que trata de reducir el número de DES implantados siguiendo esquemas anatómicos de tamaño del vaso y grado de estenosis por angiografía, este Score fue validado tanto con el uso de DES como BMS.
He dejado para el final los trabajos relacionados a la prevención de la reestenosis por vía sistémica con drogas inmunosupresoras y/o antiinflamatorios orales post implante de un BMS.
Si bien esta estrategia en la era de la angioplastia con balón no dio resultados favorables, de hecho no los podía tener dado que la fisiopatología no era inflamatoria sino producto del recoil agudo y crónico, en la era del stent metálico desnudo todos los estudios aleatorizados hechos por nosotros y por grupos europeos con drogas inmunosupresoras como la Rapamicina y/o prednisona, Alemania, Italia, Serbia y Grecia, tuvieron resultados positivos y que fueron resumidos en un meta-análisis de base de datos individuales publicado por Kastrati en el 2014, sin embargo, nunca esta estrategia fue introducida en la práctica clínica.
Nosotros en este momento estamos haciendo un estudio aleatorizado costo efectivo entre DES de última generación versus BMS más tratamiento con colchicina por tres meses solo en el grupo BMS que todavía está en la fase de reclutamiento que esperamos terminar en los próximos meses.
Dado los resultados contradictorios y de alguna manera inesperados en el largo plazo con los DES, todavía sigo creyendo que se deben explorar todas las opciones sin descartar ninguna para lograr la mayor eficacia y seguridad a mediano y largo plazo con nuestros procedimientos percutáneos de revascularización, llámese angioplastia coronaria con DES por ejemplo en bifurcaciones incluyendo probablemente todas las lesiones de tronco no protegida por el alto riesgo que llevaría la reestenosis en ese sitio, BMS en anatomías más favorables y/ o combinación de ambas estrategias.
Nada se debe descartar para lograr el mayor beneficio a nuestros pacientes y a esta especialidad que ha desvelado nuestras vidas desde su inicio.
En la última Editor Letter que escribimos en el JAMA a principios del año 2021 le decíamos a la Editora en Jefe de la Revista que creíamos importante publicar nuestra carta porque sentíamos que: “coronary angioplasty is on the cross roads”…
Necesitamos con honestidad explicar y discutir el origen de nuestros fracasos y redefinir la técnica, los “devices” y las indicaciones de otra manera solo les quedaran a las actuales y nuevas generaciones de cardiólogos intervencionistas los nichos de pacientes con infarto agudo en curso y/o pacientes terminales con contraindicación de CABG o expectativa de vida muy corta.
Muy poco para tan rica historia!!!
Referencias descriptas en el texto y recomendadas.
#-Gruentzig AR, Senning A, Siegenthaler WE. Nonoperative dilation of coronary
artery stenosis. Percutaneous transluminal coronary angioplasty.N Eng J Med 1979;301:61-8.
#-Rentrop KP, Cohen M, Hosat ST. Thrombolytic therapy in acute myocardial infarction: review of clinical trials. Am J Cardiol. 1984 Dec 21;54(11):29E-31E
#–Hartzler GO, Rutherford BD, McConahay DR et al: Percutaneous translu-minal coronary angioplasty with and without thrombolytic therapy for treatment of acute myocardial infarction. Am Heart J 1983; 106:965–973.
#- Rodríguez AE, Diaz R, Zuffardi E, Navarro P, de la Fuente LM. Angioplastia
transluminal percutánea coronaria. Rev Arg Cardiol 1982;50(2):78-91.
#. Sigwart U, Puel J, Mirkovich V, Joffre E, Kappenberger L. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty.N Eng J Med 1987;316:701-6.
#. Serruys PW, Juilliere Y, Bertrand ME, Puel J, Rickards AF, Sigwart U. Additionalimprovement of stenosis geometry in human coronary arteries by stenting after balloon dilatation. Am J Cardiol 1988 May9;61(14):71G-76G.
#. Roubin G, Gianturco C, Brown J, Robinson K, King S. Intracoronary stenting of canine coronary arteries after percutaneous coronary angioplasty. Circulation 1986;1986:74.
#. Palmaz JC, Windeler SA, Garcia F, et al. Atherosclerotic rabbit aortas: expandable intraluminal grafts. Radiology 1986;160:723-6.
# Palmaz JC. Balloon expandable intravascular stent. Am J Roentgenol 1988;150,1263-9.
#. Roubin G, Douglas JR, Lembo NJ, Black AJ, King S. Intracoronary stenting for acute closure following percutaneous coronary angioplasty. Circulation 1988;78:407.
#. Schatz RA, Baim DS, Leon M, et al. Clinical experience with the Palmaz-Schatz coronary stent. Initial result of a multicenter study. Circulation 1991;83:148-61.
#. Roubin G, Cannon AD, Agrawal SK, et al. Intracoronary stenting for acuteand threatened closure complications after transluminal coronary angioplasty. Circulation 1992; 85:916-27.
#. Sousa JE, Costa MA, Abizaid AC, et al. Sustained suppression of neointimal proliferation by sirolimus-eluting stents: one-year angiographic and intravascularultrasound follow-up. Circulation 2001 Oct 23;104(17):2007-11.
#. Rensing BJ, Vos J, Smits PC, et al. Coronary restenosis elimination with a sirolimus eluting stent: first European human experience with 6-month angiographic and intravascular ultrasonic follow-up. Eur Heart J 2001;22(22):2125-30
#Serruys PW, Degertekin M, Tanabe K, et al. RAVEL Study Group. Intravascularultrasound findings in the multicenter, randomized, double-blind RAVEL (RAndomized study with the sirolimus-eluting VElocity balloon-expandable stent in the treatment of patients with de novo native coronary artery Lesions) trial. Circulation 2002 Aug 13;106(7):798-803.
#. Grube E, Silber S, Hauptmann KE, et al. TAXUS I: six- and twelve-month results from a randomized, double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesions. Circulation 2003 Jan 7;107(1):38-42.
#. Colombo A, Drzewiecki J, Banning A, et al. TAXUS II Study Group. Randomized study to assess the effectiveness of slow- and moderate-release polymer-based paclitaxel-eluting stents for coronary artery lesions. Circulation 2003 Aug 19;108(7):788-94.
# de la Fuente LM, Miano J, Mrad J et al. Initial results of the Quanam drug eluting stent (QuaDS-QP-2) Registry (BARDDS) in human subjects. Catheter Cardiovasc Interv 2001;53(4):480-8.
#. Grube E, Lansky A, Hauptmann KE, et al. SCORE randomized trial. High-dose 7-hexanoyltaxol-eluting stent with polymer sleeves for coronary revascularization: one-year results from the SCORE randomized trial. J Am Coll Cardiol 2004 Oct 6;44(7):1368-72.
# Rodríguez AE, Santaera O, Larribau M, Sosa MI, Palacios IF. Early decrease in minimal luminal diameter after successful percutaneous transluminal coronary angioplasty predicts late restenosis. Am J Cardiol 1993;71: 1391-5.
#. Rodríguez AE, Santaera O, Larribau M et al. Coronary stenting decreases restenosis in lesions with early loss in luminal diameter 24 hours after successful PTCA. Circulation 1995;91:1397-402.
# Rodríguez A, Ayala F, Bernardi V, Santaera O, Marchand E, Pardiñas C, Mauvecin C, Vogel D, Harrell LC, Palacios IF. Optimal coronary balloon angioplasty with provisional stenting versus primary stent (OCBAS): immediate and long-term follow-up results. J Am Coll Cardiol 1998 Nov;32(5):1351-7.
#. Fischman DL, Leon MB, Baim D, et al. A randomized comparison of coronary stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501.
# Serruys PW, de Jaegere P, Kiemeneij F et al, for the BenestentStudy Group. A comparison of balloon expandable stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-95.
#. * Rodríguez A, Boullon F, Pérez Baliño N, Paviotti C, Sosa Liprandi MI, Palacios IF. Argentine Randomized Trial of Percutaneous Transluminal Coronary Angioplasty Versus Coronary Artery Bypass Surgery in Multivessel Disease (ERACI): in-hospital results and 1-year follow-up. J Am Coll Cardiol 1993;22:1060-7.
#. Hampton JR, Handerson RA, Julian DG, et al. Coronary angioplasty versus coronary artery bypass surgery: the Randomized Intervention Treatment of Angina (RITA) trial. Lancet 1993;343:573-80.
#. King SB III, Lembo NJ, Weintraub WS, et al., for the Emory Angioplasty Surgery Trial (EAST). A randomized trial comparing coronary angioplasty with coronary artery bypass surgery. N Engl J Med 1994;331:1044-50.
#. Hamm CW, Reimers J, Ischinger T, Rupprecht HJ, Berger J, Bleifeld W, for the German Angioplasty Bypass Surgery Investigation. A randomized study of coronary angioplasty compared with bypass surgery in patients with symptomaticm ultivessel coronary disease. N Engl J Med 1994;331:1037-43.
#. Rodríguez AE, Bernardi V, Navia J et al. Argentine Randomized Study: Coronary Angioplasty with Stenting versus Coronary Bypass Surgery in Patients with Multiple Vessel Disease (ERACI II): 30 days results and on year follow-up results. J Am Coll Cardiol 2001;3:51-8.
#. Serruys PW, Unger F. Sousa JE, et al. Comparison of coronary artery bypass surgery and stenting for the treatment of multi-vessel disease. N Engl J Med 2001;344:1117-24.
#. SoS Investigators Coronary Artery Bypass Surgery versus percutaneous coronary intervention with stent implantation in patients with multi-vessel coronary artery disease (the Stent or Surgery trial): a randomized controlled trial. Lancet 2002;360:965-70.
#. Hueb W, Soares P, Gersh B, et al. The Medicine, Angioplasty, or Surgery Study (MASS II trial): a randomized controlled clinical trial of three therapeutic strategies for multi-vessel coronary artery disease. J Am Coll Cardiol 2004;43:1743-51.
#. Grines CL, Cox DA, Stone GW, et al. Coronary angioplasty with or without stent implantation for acute myocardial infarction. N Engl J Med 1999; 341:1949-56.
#. Rodríguez AE, Fernández M, Santaera O et al. Coronary stenting in patients undergoing percutaneous transluminal coronary angioplasty during acute myocardial infarction. Am J Cardiol 1996 Apr 1;77(9):685-9.
#. Rodríguez AE, Bernardi V, Fernández J et al. In-hospital and late results of coronary stents versus conventional balloon angioplasty in acute myocardial infarction (GRAMI trial). Gianturco- Roubin in Acute Myocardial Infarction. Am J Cardiol 1998 Jun 1;81(11):1286-91.
#- Antoniucci D, G.M. Santoro, L. Bolognese, R. Valenti, M. Trapani, P.F. Fazzini A clinical trial comparing primary stenting of the infarct-related artery with optimal primary angioplasty for acute myocardial infarction J Am Coll Cardiol, 31 (1998), pp. 1234-1239
#. Cassese S, De Luca G, Ribichini F et al. ORAl iMmunosuppressivether apy to prevent in-Stent rEstenosiS (RAMSES) cooperation: a patient-level meta-analysis of randomized trials. Atherosclerosis 2014 Dec;237(2):410-7.
#. Hlatky MA, Boothroyd DB, Bravata DM et al.Coronary artery bypass surgery compared with percutaneous coronary interventions for multivessel disease: a collaborative analysis of individual patient data from ten randomised trials. Lancet 2009 Apr 4;373(9670):1190-7.
#. Rodríguez AE, Mieres J, Fernández-Pereira C et al. Coronary stent thrombosis in thecurrent drug-eluting stent era: insights from the ERACI III trial. J Am Coll Cardiol 2006 Jan 3;47(1):205-7. Epub 2005 Dec 9.
#. Rodríguez AE, Rodríguez-Granillo GA, Palacios IF. Late stent thrombosis the Damocles sword of Drug Eluting Stents. Eurointervention 2007 Feb; 2(4) 512-7.
#. Camenzind E, Steg PG, Wijns W. Stent thrombosis late after implantation of first-generation drug-eluting stents: a cause for concern. Circulation 2007 Mar 20;115(11):1440-55; Epub 2007 Mar 7.
# Rodríguez AE, Maree AO, Mieres J et al.Late loss of early benefit from drug eluting stents when compared with bare metal stents and coronary artery bypass surgery: 3 years follow up of ERACI III registry. Eur Heart J 2007 Sep;29 (17):2118-25.
# Rodríguez AE, Fernández-Pereira C, Rodríguez-Granillo AM.Changes in the safety paradigm with percutaneous coronary interventions in the modern era: Lessons learned from the ASCERT registry.World J Cardiol. 2012 Aug 26;4(8):242-9. doi: 10.4330/wjc.v4.i8.242.
#. Dangas GD, Farkouh ME, Sleeper LA et al, FREEDOM Investigators. Long-term outcome of PCI versus CABG in insulin and non-insulin-treated diabetic patients: results from the FREEDOM trial. J Am Coll Cardiol 2014 Sep 23;64(12):1189-97.
#. Antoniucci D, Rodríguez AE, Hempel A et al, A randomized trial comparing primary infarct artery stenting with or without abciximab in acute myocardial infarction. J Am Coll Cardiol 2003 Dec 3;42(11):1879-85.
# Waksman R, Serra A, Loh JP et al. Drug-coated balloons for de novo coronary lesions: results from the Valentines II trial. EuroIntervention 2013 Sep;9(5):613-9.
# Rodríguez AE, Vigo CF, Delacasa A et al,; EUCATAX Investigators. Efficacy and safety of a double-coated paclitaxel-eluting coronary stent: the EUCATAX trial. Catheter Cardiovasc Interv 2011Feb 15;77(3):335-42.
# Zhang JJ, Ye F, Xu K, Kan J, Tao L et al Multicentre, randomized comparison of two-stent and provisional stenting techniques in patients with complex coronary bifurcation lesions: the DEFINITION II trial. Eur Heart J. 2020 Jul 14;41(27):2523-2536
# Rodriguez AE, Fernandez-Pereira C, Mieres J, Santaera O, Antoniucci D; ERACI IV investigators. Modifying angiographic syntax score according to PCI strategy: lessons learnt from ERACI IV Study.Cardiovasc Revasc Med. 2015 Oct-Nov;16(7):418-20. doi: 10.1016/j.carrev.2015.07.001
# Rodriguez AE, Fernandez-Pereira C, Mieres J, et al Lowering risk score profile during PCI in multiple vessel disease is associated with low adverse events: The ERACI risk score.Cardiovasc Revasc Med. 2018 Oct;19(7 Pt A):792-794
# Rioufol G, Dérimay F, Roubille F,et al Fractional Flow Reserve to Guide Treatment of Patients With Multivessel Coronary Artery Disease.FUTURE Trial Investigators.J Am Coll Cardiol. 2021 Nov 9;78(19):1875-1885
# Fearon WF, Zimmermann FM, De Bruyne B et al Fractional Flow Reserve-Guided PCI as Compared with Coronary Bypass SurgeryN Engl J Med . 2021 Nov 4. doi: 10.1056/NEJMoa2112299. Online ahead of print.
# Puymirat E, Cayla G, Simon T et al Multivessel PCI Guided by FFR or Angiography for Myocardial Infarction N Engl J Med. 2021 Jul 22;385(4):297-308.,
# Gaudino, M; Hameed, I; Farkouh ME et al, Overall and Cause-Specific Mortality in Randomized Clinical Trials Comparing Percutaneous Interventions With Coronary Bypass Surgery A Meta-analysis; JAMA Intern Med. doi:10.1001/jamainternmed.2020.4748 Published online October 12, 2020.
# Rodríguez-Granillo AM, Fernández-Pereira C, Rodríguez AE.Drug-Eluting vs Bare-Metal Stents for Percutaneous Coronary Intervention. JAMA Intern Med. 2021 Jul 1;181(7):1012-1013. doi: 10.1001/jamainternmed.2021.0030.
# Head SJ, Milojevic M, Daemen J, et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet 2018;391:939–48.
# Stone GW, Kappetein AP, Sabik JF et al Five-Year Outcomes after PCI or CABG for Left Main Coronary Disease.EXCEL Trial Investigators. N Engl J Med. 2019 Nov 7;381(19):1820-1830
# Park DW, Ahn JM, Yun SC, et al. Ten-year outcomes of stents versus coronary artery bypass grafting for left main coronary artery disease. J Am Coll Cardiol 2018;72 Pt A:2813–22.
# Pavlovsky H, Rodriguez-Granillo AM, Rodriguez AE.Late Mortality After Drug-Eluting, Bare-Metal Stents, and Coronary Bypass Surgery in Left Main Disease. J Am Coll Cardiol. 2019 Apr 9;73(13):1737
# Holm NR, Mäkikallio T, Lindsay MM et al NOBLE investigators. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet. 2020 Jan 18;395(10219):191-
# Daemen J, Boersma E, Flather M et al Long-term safety and efficacy of percutaneous coronary intervention with stenting and coronary artery bypass surgery for multivessel coronary artery disease: a meta-analysis with 5-year patient-level data from the ARTS, ERACI-II, MASS-II, and SoS trials. Circulation. 2008 Sep 9;118(11):1146-54.
# Flather M, Rhee JW, Boothroyd DB et al The effect of age on outcomes of coronary artery bypass surgery compared with balloon angioplasty or bare-metal stent implantation among patients with multivessel coronary disease. A collaborative analysis of individual patient data from 10 randomized trials.J Am Coll Cardiol. 2012 Nov 20;60(21):2150-7.
# Pilgrim T, Piccolo R, Heg D et al Ultrathin-strut, biodegradable-polymer, sirolimus-eluting stents versus thin-strut, durable-polymer, everolimus-eluting stents for percutaneous coronary revascularisation: 5-year outcomes of the BIOSCIENCE randomised trial Lancet. 2018 Sep 1;392(10149):737-746.
# Hironori H, Masafumi On, Hideyuki K, et al Impact of stent length and diameter on 10-year mortality in the SYNTAXES trial Catheter Cardiovasc Interv . 2021 Sep;98(3):E379-E387.
# Gomes WJ, Albuquerque LC, Jatene FB, Leal JCF, Rocha EAV, Almeida RMS.The transfiguration of the EXCEL trial: exceeding ethical and moral boundaries.Eur J Cardiothorac Surg. 2020 Jul 1;58(1):30-34.
# Fearon WF, Zimmermann FM, De Bruyne B et al; FAME 3 Investigators.Fractional Flow Reserve-Guided PCI as Compared with Coronary Bypass Surgery. N Engl J Med. 2021 Nov 4. doi: 10.1056/NEJMoa2112299.
# Sabatine M, Bergmark B, Murphy S et al Percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting in left main coronary artery disease: an individual patient data meta-analysis Lancet. 2021 Dec 18;398(10318):2247-2257.
# Gaudino M, Hameed I, Di Franco A, Naik A, Demetres M, Biondi-Zoccai G, Bangalore S. Comparison of SYNTAX score strata effects of percutaneous and surgical revascularization trials: A meta-analysis J Thorac Cardiovasc Surg. 2021 Jun 2:S0022-5223(21)00881-3
# Piccolo R, Bonaa KH, Efthimiou O et al Drug-Eluting or Bare-Metal Stents for Left Anterior Descending or Left Main Coronary Artery Revascularization. Coronary Stent Trialists’ (CST) Collaboration. J Am Heart Assoc. 2021 Oct 19;10(20):e018828
# Correa-Sadouet C, Rodríguez-Granillo AM, Gallardo C et al; ORCA investigators. Randomized comparison between bare-metal stent plus colchicine versus drug-eluting stent alone in prevention of clinical adverse events after percutaneous coronary intervention. Protocol Future Cardiol. 2021 Jul;17(4):539-547
# Piccolo R, Bonaa KH, Efthimiou O, et al Drug-eluting or bare-metal stents for percutaneous coronary intervention: a systematic review and individual patient data meta-analysis of randomised clinical trials.Coronary Stent Trialists’ Collaboration.Lancet. 2019 Jun 22;393(10190):2503-25
# Zhang JJ, Ye F, Xu K, Kan J et al Multicentre, randomized comparison of two-stent and provisional stenting techniques in patients with complex coronary bifurcation lesions: the DEFINITION II trial. Eur Heart J. 2020 Jul 14;41(27):2523-2536
# Mieres J, Rodríguez AE, Fernández-Pereira C, Ascarrunz-Cattoretti D.Increased incidence of serious late adverse events with drug-eluting stents when compared with coronary artery bypass surgery: a cause of concern. Future Cardiol. 2020 Nov;16(6):711-723
# Valgimigli M, Campo G, Percoco et al; Multicentre Evaluation of Single High-Dose Bolus Tirofiban vs Abciximab With Sirolimus-Eluting Stent or Bare Metal Stent in Acute Myocardial Infarction Study (MULTISTRATEGY) Investigators.JAMA. 2008 Apr 16;299(15):1788-99
# Writing Committee Members, Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines J Am Coll Cardiol. 2021 Dec 7:S0735-1097(21)06157-X
# Deftereos SG, Beerkens FJ, Shah B et alColchicine in Cardiovascular Disease: In-Depth Review. Circulation. 2022 Jan 4;145(1):61-78. doi: 10.1161/CIRCULATIONAHA.121.056171.
# Matsumura-Nakano Y , Shiomi H, Morimoto T et alComparison of Outcomes of Percutaneous Coronary Intervention Versus Coronary Artery Bypass Grafting Among Patients With Three-Vessel Coronary Artery Disease in the New-Generation Drug-Eluting Stents Era (From CREDO-Kyoto PCI/CABG Registry Cohort-3) Am J Cardiol . 2021 Apr 15;145:25-36. doi: 10.1016/j.amjcard.2020.12.076.
# Toya T, Sara JD, Corban MT, Taher R et al Assessment of peripheral endothelial function predicts future risk of solid-tumor cancer Eur J Prev Cardiol. 2020 Apr;27(6):608-618.
# Abdul-Jawad Altisent,, Renier Goncalves-Ramírez L,Leticia Fernández et al Long-term Intra-coronary Structural and Vasomotor Assessment of the Absorb Bioresorbable Vascular Scaffold Am J of Cardiol . 2022 Jan 17;S0002-9149(21)01268-6. doi: 10.1016/j.amjcard.2021.12.037.
# Rajendran P, RengarajanT, Thangavel J et al The Vascular Endothelium and Human Diseases
International Journal of Biological Sciences 2013; 9(10):1057-1069
# Sidhu MS, Alexander KP, Huang Z et al Causes of Cardiovascular and Non-cardiovascular Mortality in the Ischemia Trial Originally published12 Nov 2020Circulation. 2020;142:A13030
# . Lopez-Sendon JL, Cyr DD, Mark DB et al Effects of initial invasive vs. initial conservative treatment strategies on recurrent and total cardiovascular events in the ISCHEMIA trial. Eur Heart J 2022;43:148–149.
# Rodriguez AE,Fernandez-Pereira C, Mieres J and A.Matias Rodriguez-Granillo Is non cardiac death increased with an initial invasive revascularization strategy? Commentary on the ISCHEMIA trial
European Heart Journal Open (2022) 00, 1–2 https://doi.org/10.1093/ehjopen/oeac012
La Cardiología Intervencionista que viví en mis 41 años de práctica
I wish to thank the Argentine College of interventional Cardioangiologists (CACI) for giving me the extraordinary opportunity of becoming a founding member of the College and being able to practice this medical specialty for the past 40 years. Also, I wish to extend this appreciation to the mentors behind this idea, Dr. David Vetcher, and Dr. Marcelo Ruda-Vega.
In the following pages I will try to sum up what I think are the most important experiences lived by my colleagues and I since the beginning of this medical specialty including all that has been going on in this changing and fascinating specialty. Back in 1980, I was the Cardiology/Hemodynamics/Cardiovascular Surgery unit chief resident of Sanatorio Güemes, the then called Favaloro Foundation led by directors Dr. Rene G. Favaloro, and Dr. Luis de la Fuente at the time. It was then that we came up with our first tools to perform peripheral angioplasties of both femoral and renal arteries, still without the operative and technical capabilities to start this therapy in the coronary arteries.
Almost three years had gone by since Dr. Andreas Gruntzig had presented the first cases treated in Zurich, Switzerland back in 1977 in a meeting held by the American Heart Association.
Also, by then, in 1979, Dr, Peter Rentrop had already demonstrated the benefits of intracoronary thrombolysis with streptokinase for the reperfusion patients within the first few hours after an acute myocardial infarction.
Interventional cardiology as we know it was taking off.
It was precisely on October 3, 1980—my birthday by the way—that I had my first therapeutic experience using a catheter to treat the ischemic heart disease of a patient with an ST-segment elevation myocardial infarction.
The patient had sustained a 12-hour postoperative period following a side-to-side anastomosis of venous coronary artery bypass grafts to the left anterior descending coronary and diagonal arteries that showed signs of an extensive anterolateral infarction with hemodynamic compromise.
Dr. Favaloro called the cath lab. I talked to him and suggested the possibility of infusing thrombolytic drugs in the potential occlusion site, in other words, use the saphenous vein to perform the coronary artery bypass grafting.
The famous hematologist Dr. Raúl Altman, a collaborator of Dr. Favaloro, had urokinase available because he often used it for specific treatments.
With these elements we selectively catheterized the occluding bypass, proceeded with the 1-hour in-situ infusion of urokinase, and achieved the reperfusion of the diagonal artery and the entire proximal and middle third of the left anterior descending coronary artery resulting in TIMI grade-3 flow followed by complete hemodynamic stabilization.
I gladly remember Dr. Favaloro called me and told me: «Rodriguez this is the best birthday present you’re getting this year».
I presented the case at a South American congress of cardiology, and two years later it was published as a case report in the Journal of the American Heart Association with another case performed by a different member of the Hemodynamics staff unit.
Despite I personally performed this procedure skin to skin—as we say in our day-to-day medical jargon—I was deliberately excluded from the publication without my knowledge and while on one of my numerous trips to the United States during 1981 and 1982.
Back in 1980, Dr Richard Myler, an angioplasty pioneer in the United States, was giving lectures in Sanatorio Güemes as a guest of Dr. Favaloro. The opportunity was ripe for me to join his team, which I did in January 1981 for three months. Years later, Dr. Myler introduced and inducted me as a fellow of the American College of Cardiology.
At that time, I also had the opportunity of visiting Dr. John Simpson from Stanford University who was practicing with a new steerable system of catheters and moveable core metal guidewires to perform coronary angioplasties. Back in Argentina, in April, we started performing the first coronary angioplasties at Sanatorio Güemes.
Angioplasty in Europe and the United States was on the rise with pioneers like Dr. Andreas Gruntzig from Switzerland, and one of the most notorious of all, Dr. Geoffrey Hartzler from Kansas, United States who pioneered the field of myocardial infarction angioplasty. He is one of the greatest ever, there is no doubt about that. Dr. Hartzler was, unfortunately, gone before his time, but in 1982 he introduced the method to perform primary angioplasties without previous thrombolysis (a method called direct angioplasty).
At the time, acute myocardial infarction angioplasty was very controversial with conflicting results. Also, most angioplasties were being performed after the infusion of thrombolytic drugs.
At the end of 1981, one year after having performed the aforementioned intracoronary thrombolysis, I had the opportunity to perform an angioplasty after thrombolysis on a patient with an inferior wall ST-segment elevation myocardial infarction due to right coronary artery occlusion. The first thing I did was coronary artery reperfusion with the intracoronary infusion of urokinase and then perform the balloon angioplasty. The procedure was a success.
The case was published at the beginning of 1982 in the Argentine Journal of Cardiology. To my knowledge, this was the first case of coronary angioplasty after thrombolysis ever performed in Latin America in the acute myocardial infarction setting. Probably, only a German team had performed the same procedure that same year of 1982 publishing the case in Circulation.
During the 1980s our specialty skyrockets in the entire Western world both in the United States and Europe. Also, the late 1980s see the birth of plain old balloon angioplasty (POBA) and new devices like directional coronary atherectomy, rotablation, balloon dilatation catheters, and prolonged infusions, etc. allowing us to develop more complex angioplasties than the one initially performed by Dr. Gruentzig.
It wasn’t until the mid-1980s (1986) that we created our own clinical research working group, the Cardiovascular Research Center (CECI) based on Buenos Aires, Argentina. A research center that still stands today.
At that time, the first limited but very promising experiences with bare metal stents (BMS) to prevent coronary occlusions during balloon angioplasty were beginning to take shape. Names like Dr. Sigwart, Dr. Puel, Dr. Marco, Dr. Serruys, Dr. Roubin, and Dr. Palmaz started to make a difference in all scientific settings of our specialty.
# Decades of 1990/2000/2010. The dramatic ascent of coronary angioplasty as therapeutic procedure for the management of acute and chronic coronary patients.
In my humble opinion, these were the golden decades of our medical specialty.
The first decade of 1990/2000 witnessed a consolidation in the use of bare metal stents (BMS) during angioplasty to treat acute complications and coronary restenosis after POBA to avoid chronic and acute recoil after balloon angioplasty. At the time, this was the leading cause of restenosis after this procedure. The use of BMS was first introduced in the United States by Dr. Roubin and Dr. Palmaz with their balloon-expandable stents. Dr. Gianturco-Roubin’s was the first BMS approved by the FDA in the United States to treat acute complications followed shortly after by Palmaz-Schatz’s stents .
Stents eventually would be used in all clinical conditions including the acute myocardial infarction setting and very complex coronary lesions.
Also, this decade witnesses the publication of the first randomized clinical trials on coronary angioplasty with POBA vs coronary artery bypass graft (CABG) in patients with simple obstructions of multiple vessels, most of them with chronic coronary artery disease, also in diabetic patients. Shortly after these same comparisons would be made with the use of BMS . This is also the time when the first comparative randomized trials on acute myocardial infarctions treated with angioplasty vs thrombolysis are published followed by studies on angioplasty with POBA vs angioplasty with stenting .
During this decade two landmark meta-analyses confirmed that, in the long run, the angioplasty in patients with multivessel disease has the same survival and infarction-free survival rates compared to CABG excluding diabetic patients. In these analyses the survival rate of young patients showed a clear advantage towards the angioplasty, which is comprehensible, but was confirmed in this meta-analysis for the first time. The only difference in favor of CABG was the higher rate of new requirements for angioplasty revascularization.
Unfortunately, these findings were published,2008-2009, just when drug-eluting stents (DES) were on the rise, which is why these results were overlooked.
Although the use of bare metal stents minimized the occurrence of acute complications after angioplasty, it also caused in-stent restenosis due to fibrous intimal hyperplasia following the exaggerated scarring caused by new reinterventions of the target vessel within the first 8 to 10 months after stenting (> 20% rate).
The introduction of immunosuppressive drugs within the stent to be released in the arterial endothelium within the first month after stenting caused a significant reduction of this hyperplasia followed by a significant reduction of new revascularizations. Also, this combination prevented acute recoil and fibrous intimal hyperplasia.
This marked the beginning of DES that revolutionized our medical specialty. Actually, to this date, in certain discussion fora—not mine—they still revolutionize our specialty.
Esto es el inicio de los stents liberadores de fármacos (DES) que revolucionaron y aun hoy en algunos foros de discusión, no en el mío propio, siguen revolucionando nuestra especialidad. The names of Antonio Colombo, Eberhard Grube, Martin Leon, Patrick W. Serruys and Greg Stone are largely due to them this technological leap with the introduction of drug-eluting stents (DES). At this point, our colleague Eduardo Sousa and his group in Brazil also played an important role. However, our country was again not absent in this development of deS, and one of the observational studies in its use was carried out in Argentina by Dr Luis de la Fuente and despite the fact that his findings were not endorsed by a long multinational randomized European study, which had to be terminated prematurely due to excess of thrombotic complications of this DES design, this pilot study was pioneering at the time.
The significant reduction of new revascularizations reported after DES implantation brought expectations that were a little too optimistic regarding the use of stents like this. Rumor had it that «the end of restenosis would also be the end of CABG» following the early findings from the first randomized clinical trials on the use of DES. In the following section we will see how far we still are from these predictions.
This overoptimistic approach was built on reducing completely secondary and non-clinical endpoints to a minimum like minimizing the so-called “late loss” that could never be associated with the occurrence of hard endpoints after angioplasty.
# Decade of 2010/2021. The dramatic ascent of the indication of revascularization to the present day.
At this point I want to be very straightforward, but also very critical, and my opinions should also be taken from this personal point of view.
With the arrival of DES into the routine clinical practice, to this date, several randomized clinical trials including comparison groups have been conducted on angioplasty with DES vs CABG. As a matter of fact, up to 3 studies on unprotected left main coronary artery disease, 1 on multiple vessels and left main coronary artery, and the remaining 4 on multiple vessels including diabetic patients have been conducted.
From the beginning, all trials but 1 invariably showed more revascularization procedures as a natural companion of the angioplasty, which should not worry us. However, in 7 of these trials, the mortality and/or spontaneous myocardial infarction rates also went up, which is more disturbing and is associated with mortality.
The greater complexity of the patients treated could explain these findings, but it is probably not the only hypothesis. As a matter of fact, several meta-analyses proved that regardless of the anatomical complexity, the rate of hard endpoints like myocardial infarction—and in some studies, mortality—was lower with CABG.
This change in safety parameters in comparative studies with surgery had already been observed in the long American registry of ASCERT with 190 thousand patients treated with CABG and PCI (78% DES1) during the years 2004 to 2008 in 64 sites in the USA and where in patients >64 years there was a significant reduction in mortality with CABG even in groups of low angiographic and clinical risk (non-diabetic and two-vessel injury). and what a reason why we wrote a review article in 2012, where we already drew attention to these findings. This reference is among the suggested articles to read.
Although it is completely true that DES reduced significantly the rate of new revascularizations, mortality did not change when the old DES and/or even BMS designs were compared to the new ones.
With the first designs, the use of DES had 4 limitations some of which overlap:
1- Early, late, and very late stent thrombosis.
2- Poor late DES apposition. These 2 overlapped most of the times.
3- Early neo-atherosclerosis immediately after implantation (beyond 1st year).
4- Endothelial dysfunction both in the stent and in the proximal and distal segments of the implant.
Stent thrombosis and poor stent apposition were significantly associated with the polymer, but, to this date, this is not a problem anymore.
However, the 2 remaining ones—early neo-atherosclerosis and endothelial dysfunction—were mainly associated with the local action of the immunosuppressant drug. The former causes spontaneous infarctions not associated with new procedures that we have been invariably seeing in all randomized trials including comparison groups on CABG. Endothelial dysfunction is also associated with cardiac adverse events, but ultimately with non-cardiac adverse events too including a higher incidence rate of solid tumors.
It should not be forgotten that the endothelium is an organ with multiple functions such as: «vasodilation, thrombolysis, platelet disagreggation, antioxidant, antiinflammation, antiproliferation». The loss of its normal function i.e. endothelial dysfunction could produce the opposite effects: «vasocontriction, thrombosis, platelet agreggation, oxidant activity, inflammation and growth factors». At this point it is very important that interventional cardiologists define cost/benefit between suppression of restenosis / endothelial dysfunction and the clinical implications of the last one.
On this topic I recommend reading the manuscripts referenced below by Toya et al. and Abdul-Jawad Altisent et al., within the last references in this chapter.
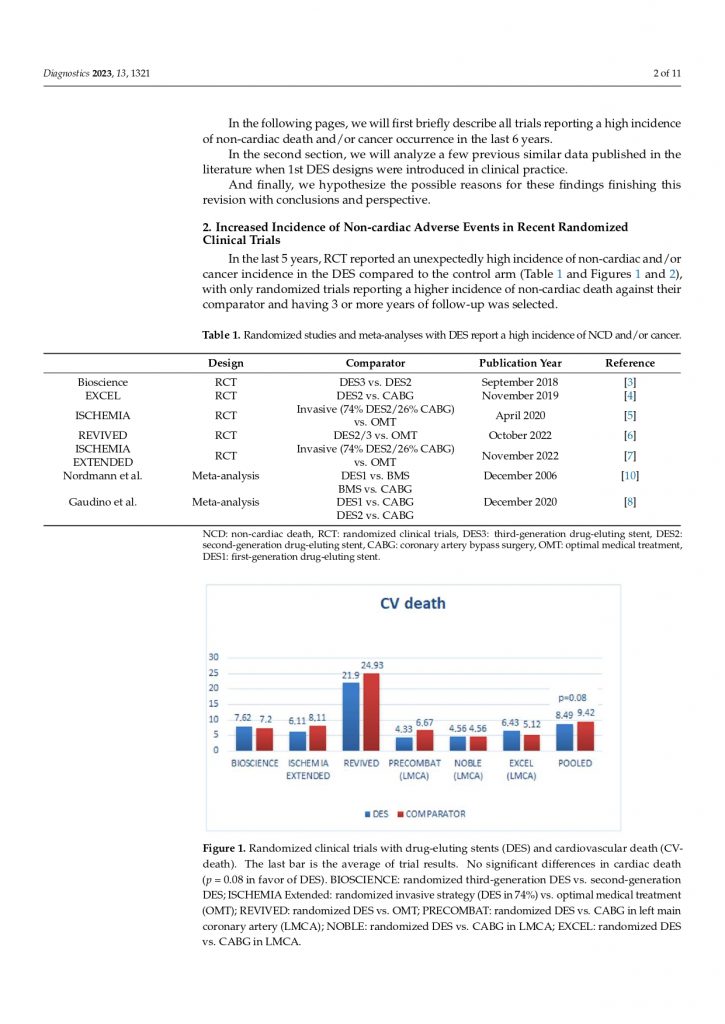
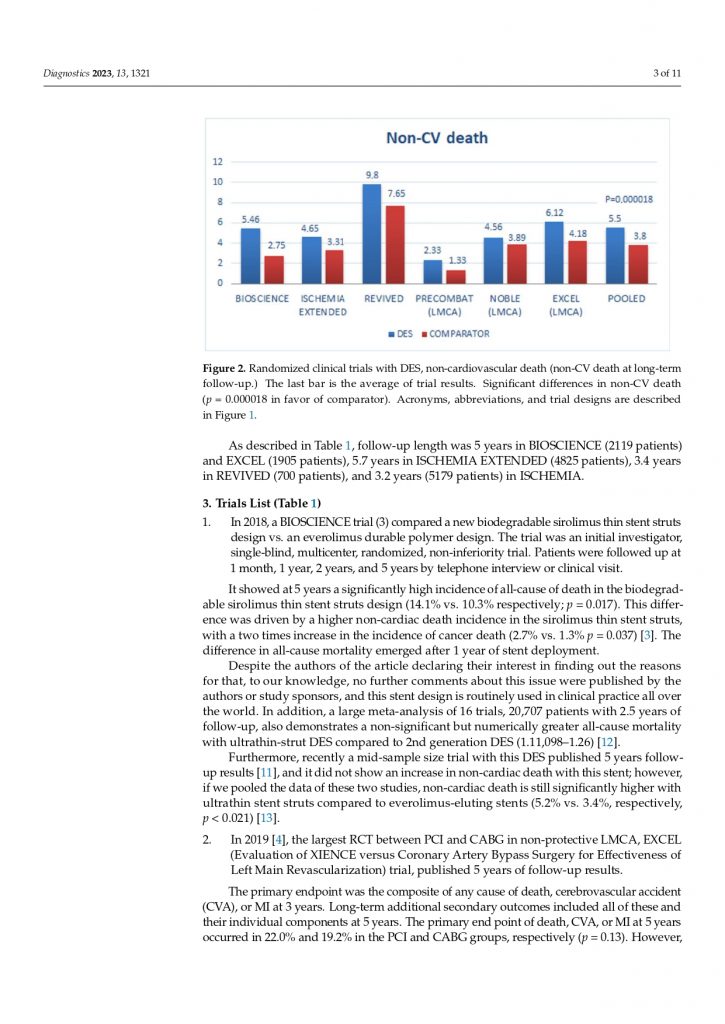
It is surprising to see several observations associated with non-cardiac mortality in patients treated with angioplasty at the present time who were not in previous observations. Actually, this should be a cause for careful analysis in properly conducted randomized clinical trials and prospective registries. This increased non-cardiac mortality was reported not only in randomized clinical trials on DES and CABG, but also in comparisons of different DES designs. As we already know, large enough randomized clinical trials have the power to homogenize populations at a baseline level, which is why the explanation to this increased mortality should be looked for in other clinical settings. I recommend reading Gaudino’s meta-analysis, the 5 years of EXCEL trial, Pilgrim’s et al 5-year study of an «ultrathin DES», the CREDO-Kyoto registry of angioplasties and CABG all referenced below as well as the abstract of the ISCHEMIA trial published in Circulation in November of last year and the European Heart Journal this year. The publication of the last one was the reason of an Editorial comment of ours that is published in the European Heart Journal Open in February of this year and where in a Table we describe all the studies that reported an increase in non-cardiac death with DES in long-term follow-up, to these we must include the findings of the ISCHEMIA study that is really very worrying.
In my opinion calling non-cardiac mortality an adverse event due to coincidence is reckless, illogical, and eventually hurts our own medical specialty.
Only after a sincere discussion of all these findings with opinion leaders and industry CEOs we will be able to escape this labyrinth we fall into with every new randomized trial on CABG or with every medical therapy that only brings us frustration.
Lately even the introduction of methods of functional diagnosis of coronary lesions such as FFR or iFR to guide PCI have not been successful in demonstrating reduction of post-implantation events of DES both in patients with acute infarction or elective patients. I recommend reading the results published this year of randomized studies in this regard including FUTURE, FAME 3 and that of Puymirat E et al in acute myocardial infarction all referenced below between the suggested readings. The negative results of these studies with FFR show us that quickly interventional cardiologists adopt techniques and new «devices» often generating false expectations due to a hasty overestimation of the benefits.
Although the recently published new clinical guidelines on therapeutics elaborated together with clinical cardiologists are somehow benevolent to our medical specialty, they show that, unlike we thought 15 years ago, despite the arrival of state-of-the-art DES designs, coronary artery bypass grafting is more alive than ever. In fact, both American (USA) and European Societies of Cardiovascular and Thoracic surgery didn’t endorse that guideline.
# Creation of the Cardiovascular Research Center (CECI).
In 1986 together with colleagues and friends we formed an independent working group first in the Anchorena Sanatorium and then moved to the Otamendi Sanatorium from 1993 to the present.
During all these years there are no words to describe the support for all our care and scientific tasks developed in the Otamendi, so my thanks to your past authorities Drs. Jose A. De All for whoever comes to work in this Institution and Dr Jorge Aufiero as well as the current authorities.
During all these years, many cardiologists went through the Service to be trained in the practice of our specialty, many of them today Heads of Service in reference places in our country as well as prominent members of scientific societies that could not list them by the quantity, both in our country and in Latin America. Residents of almost all nationalities of the Spanish- and Portuguese-speaking region passed through the service from Paraguay, Chile, Brazil, Bolivia, Peru, Uruguay, Ecuador, Venezuela, Colombia, Panama and the Dominican Republic who then continued to be connected with us, often carrying out joint research work.
Back in 1988, two years after creating a working group with friends and colleagues, we teamed up again to create an independent department of clinical research. Although it was not created as a CRO (there are several examples of excellent CROs in Argentina), it allowed us to arrange multiple research protocols in our country in an orderly fashion, and one by one at the beginning. Afterwards, we conducted multicenter studies including international clinical trials.
Here is a summary of the most significant clinical trials conducted that I think played a key role in our routine clinical practice:
This whole thing started with the first randomized clinical trial published on coronary angioplasty with POBA vs CABG—the ERACI I trial—published in JACC in 1993 and 1995. Years later with the arrival of BMS, the second version of this study, the ERACI II, was published. Unlike the ERACI I, this multicenter trial was co-authored by the fondly remembered Dr. Liliana Grinfeld. Both manuscripts were published in JACC in 2001 and 2005 including the 1- and 5-year follow-up simultaneously published with Dr. Patrick Serruys’ ARTS study.
Back in 1993, we published an observation suggesting that restenosis after balloon angioplasty was mainly due to acute artery recoil after balloon dilatation. Something completely new that we had never associated. In the animal model of restenosis common knowledge was that the endothelial damage due to the mechanism of the angioplasty triggered vessel restenosis months later. However, this was not the case with human beings in whom atherosclerotic plaque is often eccentric and behaves different from the balloon in such a way that the rate of restenosis was very low in lesions whose diameter did not change 24 hours after balloon angioplasty. This finding was published in several scientific journals: American Journal of Cardiology in 1993 and 1995, Circulation in 1995, and JACC in 1998 and also of academic discussions with world opinion leaders since they spoke of: «.. coronary restenosis a time related phenomenom…» therefore our observations were totally opposite and were the subject of controversy. Time proved us right and Patrick Serruys ended up accepting that acute recoil was a very important phenomenon in the pathophysiology of post POBA restenosis, there he began talking about «stent like results post POBA» in other words optimal post-balloon results without acute recoil.
It was very pleasant 3 years ago to see in the gallery of the PCR Congress exposed as one of the milestones of angioplasty precisely the work of our stent in elastic recoil OCBAS trial that was published in JACC 1998 together with the ERACI I and II studies.
In the same sense, it was also very pleasant to read in the book on the history of cardiovascular interventions and interventional cardiology that one of its greatest pioneers Gary Roubin whose aforementioned book was entitled «The First Balloon-Expandable Coronary Stent an Expedition That Changed Cardiovascular Medicine» published in 2015 included us along with Julio Palmaz and Rene Favaloro as the only Latin Americans in the list of the 93 pioneers of Angioplasty and Cardiovascular Interventions, this reference is also within the suggested lectures of this chapter.
The use of stent in the acute myocardial infarction setting is appealing but was also very controversial too. Together with the beloved Dr. Gary Roubin our group published a short experience on the use of stent in the ST-segment elevation myocardial infarction setting in the American Journal of Cardiology back in 1996. This experience immediately turned into the first study on the use of stents in the acute myocardial infarction setting accepted for publication. The GRAMI trial—published in the American Journal of Cardiology in 1998—was contemporaneous to Dr. David Antoniucci’s study. Actually, his study was published two months prior to the JACC publication, but ours had already been accepted two months before the Florence study. Therefore, both chronologically and academically we came first. Anecdotes I always like to remember in our family reunions with my great Italian friend.
Already in the new millennium, the CECI Center participated in prospective records and observational studies such as those related to DES thrombosis published in EuroIntervention in February 2007 («Late stent thrombosis the Damocles sword of DES») a month before the promoted article by Camenzid and Wijns in Circulation, the ERACI III record, which was published in JACC in 2006 and in the Eur Heart J in 2007 this last work was one of the reason why this European Journal will increase its «impact factor» according to a personal letter we received from the Editor-in-Chief of that Journal.
The review article on «DES late thrombosis» there were friends who recommended me not to publish it because it could have adverse reactions from the industry that manufactured the DES, despite those tips, the work was sent and then review accepted and published in EuroIntervention. I must also say that I never felt an adverse reaction from the industry for this.
If the doctors of the CACI specialty career wonder how we were able from Argentina to carry out so many studies that were published in the largest English-speaking «Journals» I would tell them that everything is achieved with work and a lot of honesty in the analysis and observation of the facts that one is seeing. You should always be sure of what you are saying, and you should always check the information several times before making a further judgment if this implies original findings outside of what is established and expected. In fact, at the time where these thoughts were writing, February 20th, 2022, according Research Gate scientific data manuscripts published by us as authors or coauthors deserved 25320 reads,7462 citations and have 3862 points of research interest the largest numbers achieve by any group or individual person in our country in the area of interventional cardiology.
Controversies with our findings happened in several times, with the «elastic recoil», the ERACI studies and with stent in acute myocardial infarction. In these points the collaboration with Igor Palacios, Gary Roubin, John Ambrose, William O’Neill and David Antoniucci were very important. As I said on the occasion of a distinction granted to me by the Legislature of CABA: » the work we did here in Argentina with ideas totally ours and our patients, but nothing would have been the same if our friend from USA or EU didn’t support to us «.
In the ERACI I study, which Favaloro was very angry when we did and spoke ill of the findings including trying to convince the surgeon who had operated on almost all patients not to sign the manuscript once it was approved in the JACC, an Argentine work published in the JACC in 1993 had few precedents in the cardiology of our country, finally cousin rationality and the surgeon signed the work, Dr Néstor Perez-Balino was a faithful witness of what I am recounting. I had, however, the pleasure that several years later, in May 2000, when the new ERACI II had already been accepted for publication, Favaloro called me by phone to congratulate me personally on this work and with warm memories of the past shared in a very difficult moment of the Foundation and also personal of him few months before his death.
Over the last 20 years, the Cardiovascular Research Center (CECI) has conducted several multinational and randomized clinical trials on several DES designs and different revascularization strategies in patients with acute myocardial infarction, as well as in chronic patients.
In this way we participate in the abciximab in acute infarction with a carbon metal stent, JESTENT rheolithic thrombectomy in acute infarction, FREEDOM, FREEDOM long term outcome DES vs CABG in diabetic patients, MULTISTRATEGY on DES and abciximab in acute infarction, VALENTINES with Paclitaxel releasing balloon, DEFINITION II treatment of bifurcations with DES including lesions of unprotected trunk and lately MASTER DAPT comparison of antiplatelet strategy with DES, all of them published several times in NEJM, JAMA, JACC, Circulation, Eur Heart Journal, JACC Intervention and EuroIntervention
Similarly, our database was submitted for analysis and control through several meta-analyses, and eventually, the ERACI and ERACI II clinical trials were submitted for publication (Dr. Pocok in The Lancet, 1995; Dr. Hlatky in The Lancet, 2009 and JACC in 2012; Dr. Daemen in Circulation, 2008, and Dr. Head in The Lancet back in 2018).
Likewise, the database of the EUCATAX trial was submitted to Dr. Valgimigli for the publication of his meta-analysis in The Lancet in 2019, and Circulation in 2021.
Also, based on a prospective registry of multiple vessels, is that the ERACI Score was born as a revascularization strategy in patients with multi-vessel disease and left coronary trunk, which was a joint product of several centers in our country and that tries to reduce the number of DES implanted following anatomical schemes of vessel size and degree of stenosis by angiography, this Score was validated with both the use of DES and BMS.
Last but not least, the studies on the systemic prevention of restenosis with oral immunosuppressant and anti-inflammatory agents after BMS implantation.
Although in the era of balloon angioplasty this strategy did not had favorable results—as a matter of fact no positive results could come from it because the pathophysiology was not inflammatory—in the era of bare metal stents all the randomized clinical trials conducted by us and European working groups in Germany, Italy, Serbia, and Greece on immunosuppressant drugs like rapamycin and/or prednisone had positive results that were summed up in a meta-analysis published by Dr. Kastrati in 2014. Still this strategy was never part of the routine clinical practice.
At this moment, we are conducting a cost-effective randomized clinical trial between state-of-the-art DES vs BMS plus a 3-month course of colchicine only in the BMS group that is still in the recruiting phase. We can only hope it will be completed in the next months.
Given the conflicting and somehow unexpected long-term results with DES, I still believe all options should be on the table and none should be discarded to achieve a greater mid- and long-term efficacy and safety with our percutaneous revascularization procedures whether coronary angioplasty with DES implantation in bifurcation lesions probably including most of unprotected left main coronary artery disease, and BMS implantation in more favorable anatomies, and/or a combination of both strategies.
Nothing should be left out if we want our patients to benefit the most, and if we want to improve this medical specialty that has shaped our lives for so long.
In the last Editor Letter we wrote at JAMA at the beginning of 2021 we told the Editor-in-Chief of the Journal that we thought it was important to publish our letter because we felt that: ….»coronary angioplasty is on the cross roads«…
We need to honestly explain and discuss the origin of our failures and redefine the technique, the «devices» and the indications in another way only the current and new generations of interventional cardiologists will have the niches of patients with acute infarction in progress and / or terminal patients with contraindication of CABG or very short life expectance.
Very little for such a rich history!!!
References suggested
#-Gruentzig AR, Senning A, Siegenthaler WE. Nonoperative dilation of coronary
artery stenosis. Percutaneous transluminal coronary angioplasty.N Eng J Med 1979;301:61-8.
#-Rentrop KP, Cohen M, Hosat ST. Thrombolytic therapy in acute myocardial infarction: review of clinical trials. Am J Cardiol. 1984 Dec 21;54(11):29E-31E
#–Hartzler GO, Rutherford BD, McConahay DR et al: Percutaneous translu-minal coronary angioplasty with and without thrombolytic therapy for treatment of acute myocardial infarction. Am Heart J 1983; 106:965–973.
#- Rodríguez AE, Diaz R, Zuffardi E, Navarro P, de la Fuente LM. Angioplastia
transluminal percutánea coronaria. Rev Arg Cardiol 1982;50(2):78-91.
#. Sigwart U, Puel J, Mirkovich V, Joffre E, Kappenberger L. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty.N Eng J Med 1987;316:701-6.
#. Serruys PW, Juilliere Y, Bertrand ME, Puel J, Rickards AF, Sigwart U. Additionalimprovement of stenosis geometry in human coronary arteries by stenting after balloon dilatation. Am J Cardiol 1988 May9;61(14):71G-76G.
#. Roubin G, Gianturco C, Brown J, Robinson K, King S. Intracoronary stenting of canine coronary arteries after percutaneous coronary angioplasty. Circulation 1986;1986:74.
#. Palmaz JC, Windeler SA, Garcia F, et al. Atherosclerotic rabbit aortas: expandable intraluminal grafts. Radiology 1986;160:723-6.
# Palmaz JC. Balloon expandable intravascular stent. Am J Roentgenol 1988;150,1263-9.
#. Roubin G, Douglas JR, Lembo NJ, Black AJ, King S. Intracoronary stenting for acute closure following percutaneous coronary angioplasty. Circulation 1988;78:407.
#. Schatz RA, Baim DS, Leon M, et al. Clinical experience with the Palmaz-Schatz coronary stent. Initial result of a multicenter study. Circulation 1991;83:148-61.
#. Roubin G, Cannon AD, Agrawal SK, et al. Intracoronary stenting for acuteand threatened closure complications after transluminal coronary angioplasty. Circulation 1992; 85:916-27.
#. Sousa JE, Costa MA, Abizaid AC, et al. Sustained suppression of neointimal proliferation by sirolimus-eluting stents: one-year angiographic and intravascularultrasound follow-up. Circulation 2001 Oct 23;104(17):2007-11.
#. Rensing BJ, Vos J, Smits PC, et al. Coronary restenosis elimination with a sirolimus eluting stent: first European human experience with 6-month angiographic and intravascular ultrasonic follow-up. Eur Heart J 2001;22(22):2125-30
#Serruys PW, Degertekin M, Tanabe K, et al. RAVEL Study Group. Intravascularultrasound findings in the multicenter, randomized, double-blind RAVEL (RAndomized study with the sirolimus-eluting VElocity balloon-expandable stent in the treatment of patients with de novo native coronary artery Lesions) trial. Circulation 2002 Aug 13;106(7):798-803.
#. Grube E, Silber S, Hauptmann KE, et al. TAXUS I: six- and twelve-month results from a randomized, double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesions. Circulation 2003 Jan 7;107(1):38-42.
#. Colombo A, Drzewiecki J, Banning A, et al. TAXUS II Study Group. Randomized study to assess the effectiveness of slow- and moderate-release polymer-based paclitaxel-eluting stents for coronary artery lesions. Circulation 2003 Aug 19;108(7):788-94.
# de la Fuente LM, Miano J, Mrad J et al. Initial results of the Quanam drug eluting stent (QuaDS-QP-2) Registry (BARDDS) in human subjects. Catheter Cardiovasc Interv 2001;53(4):480-8.
#. Grube E, Lansky A, Hauptmann KE, et al. SCORE randomized trial. High-dose 7-hexanoyltaxol-eluting stent with polymer sleeves for coronary revascularization: one-year results from the SCORE randomized trial. J Am Coll Cardiol 2004 Oct 6;44(7):1368-72.
# Rodríguez AE, Santaera O, Larribau M, Sosa MI, Palacios IF. Early decrease in minimal luminal diameter after successful percutaneous transluminal coronary angioplasty predicts late restenosis. Am J Cardiol 1993;71: 1391-5.
#. Rodríguez AE, Santaera O, Larribau M et al. Coronary stenting decreases restenosis in lesions with early loss in luminal diameter 24 hours after successful PTCA. Circulation 1995;91:1397-402.
# Rodríguez A, Ayala F, Bernardi V, Santaera O, Marchand E, Pardiñas C, Mauvecin C, Vogel D, Harrell LC, Palacios IF. Optimal coronary balloon angioplasty with provisional stenting versus primary stent (OCBAS): immediate and long-term follow-up results. J Am Coll Cardiol 1998 Nov;32(5):1351-7.
#. Fischman DL, Leon MB, Baim D, et al. A randomized comparison of coronary stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501.
# Serruys PW, de Jaegere P, Kiemeneij F et al, for the BenestentStudy Group. A comparison of balloon expandable stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-95.
#. * Rodríguez A, Boullon F, Pérez Baliño N, Paviotti C, Sosa Liprandi MI, Palacios IF. Argentine Randomized Trial of Percutaneous Transluminal Coronary Angioplasty Versus Coronary Artery Bypass Surgery in Multivessel Disease (ERACI): in-hospital results and 1-year follow-up. J Am Coll Cardiol 1993;22:1060-7.
#. Hampton JR, Handerson RA, Julian DG, et al. Coronary angioplasty versus coronary artery bypass surgery: the Randomized Intervention Treatment of Angina (RITA) trial. Lancet 1993;343:573-80.
#. King SB III, Lembo NJ, Weintraub WS, et al., for the Emory Angioplasty Surgery Trial (EAST). A randomized trial comparing coronary angioplasty with coronary artery bypass surgery. N Engl J Med 1994;331:1044-50.
#. Hamm CW, Reimers J, Ischinger T, Rupprecht HJ, Berger J, Bleifeld W, for the German Angioplasty Bypass Surgery Investigation. A randomized study of coronary angioplasty compared with bypass surgery in patients with symptomaticm ultivessel coronary disease. N Engl J Med 1994;331:1037-43.
#. Rodríguez AE, Bernardi V, Navia J et al. Argentine Randomized Study: Coronary Angioplasty with Stenting versus Coronary Bypass Surgery in Patients with Multiple Vessel Disease (ERACI II): 30 days results and on year follow-up results. J Am Coll Cardiol 2001;3:51-8.
#. Serruys PW, Unger F. Sousa JE, et al. Comparison of coronary artery bypass surgery and stenting for the treatment of multi-vessel disease. N Engl J Med 2001;344:1117-24.
#. SoS Investigators Coronary Artery Bypass Surgery versus percutaneous coronary intervention with stent implantation in patients with multi-vessel coronary artery disease (the Stent or Surgery trial): a randomized controlled trial. Lancet 2002;360:965-70.
#. Hueb W, Soares P, Gersh B, et al. The Medicine, Angioplasty, or Surgery Study (MASS II trial): a randomized controlled clinical trial of three therapeutic strategies for multi-vessel coronary artery disease. J Am Coll Cardiol 2004;43:1743-51.
#Roubin GS The First Balloon Expandable Coronary Stent, An Expedition that change Cardiovascular Medicine: A Memoir. University of Queensland Press, St Lucia Queesnland, Australia 2014
#. Grines CL, Cox DA, Stone GW, et al. Coronary angioplasty with or without stent implantation for acute myocardial infarction. N Engl J Med 1999; 341:1949-56.
#. Rodríguez AE, Fernández M, Santaera O et al. Coronary stenting in patients undergoing percutaneous transluminal coronary angioplasty during acute myocardial infarction. Am J Cardiol 1996 Apr 1;77(9):685-9.
#. Rodríguez AE, Bernardi V, Fernández J et al. In-hospital and late results of coronary stents versus conventional balloon angioplasty in acute myocardial infarction (GRAMI trial). Gianturco- Roubin in Acute Myocardial Infarction. Am J Cardiol 1998 Jun 1;81(11):1286-91.
#- Antoniucci D, G.M. Santoro, L. Bolognese, R. Valenti, M. Trapani, P.F. Fazzini A clinical trial comparing primary stenting of the infarct-related artery with optimal primary angioplasty for acute myocardial infarction J Am Coll Cardiol, 31 (1998), pp. 1234-1239
#. Cassese S, De Luca G, Ribichini F et al. ORAl iMmunosuppressivether apy to prevent in-Stent rEstenosiS (RAMSES) cooperation: a patient-level meta-analysis of randomized trials. Atherosclerosis 2014 Dec;237(2):410-7.
#. Hlatky MA, Boothroyd DB, Bravata DM et al.Coronary artery bypass surgery compared with percutaneous coronary interventions for multivessel disease: a collaborative analysis of individual patient data from ten randomised trials. Lancet 2009 Apr 4;373(9670):1190-7.
#. Rodríguez AE, Mieres J, Fernández-Pereira C et al. Coronary stent thrombosis in thecurrent drug-eluting stent era: insights from the ERACI III trial. J Am Coll Cardiol 2006 Jan 3;47(1):205-7. Epub 2005 Dec 9.
#. Rodríguez AE, Rodríguez-Granillo GA, Palacios IF. Late stent thrombosis the Damocles sword of Drug Eluting Stents. Eurointervention 2007 Feb; 2(4) 512-7.
#. Camenzind E, Steg PG, Wijns W. Stent thrombosis late after implantation of first-generation drug-eluting stents: a cause for concern. Circulation 2007 Mar 20;115(11):1440-55; Epub 2007 Mar 7.
# Rodríguez AE, Maree AO, Mieres J et al.Late loss of early benefit from drug eluting stents when compared with bare metal stents and coronary artery bypass surgery: 3 years follow up of ERACI III registry. Eur Heart J 2007 Sep;29 (17):2118-25.
# Rodríguez AE, Fernández-Pereira C, Rodríguez-Granillo AM.Changes in the safety paradigm with percutaneous coronary interventions in the modern era: Lessons learned from the ASCERT registry.World J Cardiol. 2012 Aug 26;4(8):242-9. doi: 10.4330/wjc.v4.i8.242.
#. Dangas GD, Farkouh ME, Sleeper LA et al, FREEDOM Investigators. Long-term outcome of PCI versus CABG in insulin and non-insulin-treated diabetic patients: results from the FREEDOM trial. J Am Coll Cardiol 2014 Sep 23;64(12):1189-97.
#. Antoniucci D, Rodríguez AE, Hempel A et al, A randomized trial comparing primary infarct artery stenting with or without abciximab in acute myocardial infarction. J Am Coll Cardiol 2003 Dec 3;42(11):1879-85.
# Waksman R, Serra A, Loh JP et al. Drug-coated balloons for de novo coronary lesions: results from the Valentines II trial. EuroIntervention 2013 Sep;9(5):613-9.
# Rodríguez AE, Vigo CF, Delacasa A et al,; EUCATAX Investigators. Efficacy and safety of a double-coated paclitaxel-eluting coronary stent: the EUCATAX trial. Catheter Cardiovasc Interv 2011Feb 15;77(3):335-42.
# Zhang JJ, Ye F, Xu K, Kan J, Tao L et al Multicentre, randomized comparison of two-stent and provisional stenting techniques in patients with complex coronary bifurcation lesions: the DEFINITION II trial. Eur Heart J. 2020 Jul 14;41(27):2523-2536
# Rodriguez AE, Fernandez-Pereira C, Mieres J, Santaera O, Antoniucci D; ERACI IV investigators. Modifying angiographic syntax score according to PCI strategy: lessons learnt from ERACI IV Study.Cardiovasc Revasc Med. 2015 Oct-Nov;16(7):418-20. doi: 10.1016/j.carrev.2015.07.001
# Rodriguez AE, Fernandez-Pereira C, Mieres J, et al Lowering risk score profile during PCI in multiple vessel disease is associated with low adverse events: The ERACI risk score.Cardiovasc Revasc Med. 2018 Oct;19(7 Pt A):792-794
# Rioufol G, Dérimay F, Roubille F,et al Fractional Flow Reserve to Guide Treatment of Patients With Multivessel Coronary Artery Disease.FUTURE Trial Investigators.J Am Coll Cardiol. 2021 Nov 9;78(19):1875-1885
# Fearon WF, Zimmermann FM, De Bruyne B et al Fractional Flow Reserve-Guided PCI as Compared with Coronary Bypass SurgeryN Engl J Med . 2021 Nov 4. doi: 10.1056/NEJMoa2112299. Online ahead of print.
# Puymirat E, Cayla G, Simon T et al Multivessel PCI Guided by FFR or Angiography for Myocardial Infarction N Engl J Med. 2021 Jul 22;385(4):297-308.,
# Gaudino, M; Hameed, I; Farkouh ME et al, Overall and Cause-Specific Mortality in Randomized Clinical Trials Comparing Percutaneous Interventions With Coronary Bypass Surgery A Meta-analysis; JAMA Intern Med. doi:10.1001/jamainternmed.2020.4748 Published online October 12, 2020.
# Rodríguez-Granillo AM, Fernández-Pereira C, Rodríguez AE.Drug-Eluting vs Bare-Metal Stents for Percutaneous Coronary Intervention. JAMA Intern Med. 2021 Jul 1;181(7):1012-1013. doi: 10.1001/jamainternmed.2021.0030.
# Head SJ, Milojevic M, Daemen J, et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet 2018;391:939–48.
# Stone GW, Kappetein AP, Sabik JF et al Five-Year Outcomes after PCI or CABG for Left Main Coronary Disease.EXCEL Trial Investigators. N Engl J Med. 2019 Nov 7;381(19):1820-1830
# Park DW, Ahn JM, Yun SC, et al. Ten-year outcomes of stents versus coronary artery bypass grafting for left main coronary artery disease. J Am Coll Cardiol 2018;72 Pt A:2813–22.
# Pavlovsky H, Rodriguez-Granillo AM, Rodriguez AE.Late Mortality After Drug-Eluting, Bare-Metal Stents, and Coronary Bypass Surgery in Left Main Disease. J Am Coll Cardiol. 2019 Apr 9;73(13):1737
# Holm NR, Mäkikallio T, Lindsay MM et al NOBLE investigators. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet. 2020 Jan 18;395(10219):191-
# Daemen J, Boersma E, Flather M et al Long-term safety and efficacy of percutaneous coronary intervention with stenting and coronary artery bypass surgery for multivessel coronary artery disease: a meta-analysis with 5-year patient-level data from the ARTS, ERACI-II, MASS-II, and SoS trials. Circulation. 2008 Sep 9;118(11):1146-54.
# Flather M, Rhee JW, Boothroyd DB et al The effect of age on outcomes of coronary artery bypass surgery compared with balloon angioplasty or bare-metal stent implantation among patients with multivessel coronary disease. A collaborative analysis of individual patient data from 10 randomized trials.J Am Coll Cardiol. 2012 Nov 20;60(21):2150-7.
# Pilgrim T, Piccolo R, Heg D et al Ultrathin-strut, biodegradable-polymer, sirolimus-eluting stents versus thin-strut, durable-polymer, everolimus-eluting stents for percutaneous coronary revascularisation: 5-year outcomes of the BIOSCIENCE randomised trial Lancet. 2018 Sep 1;392(10149):737-746.
# Hironori H, Masafumi On, Hideyuki K, et al Impact of stent length and diameter on 10-year mortality in the SYNTAXES trial Catheter Cardiovasc Interv . 2021 Sep;98(3):E379-E387.
# Gomes WJ, Albuquerque LC, Jatene FB, Leal JCF, Rocha EAV, Almeida RMS.The transfiguration of the EXCEL trial: exceeding ethical and moral boundaries.Eur J Cardiothorac Surg. 2020 Jul 1;58(1):30-34.
# Fearon WF, Zimmermann FM, De Bruyne B et al; FAME 3 Investigators.Fractional Flow Reserve-Guided PCI as Compared with Coronary Bypass Surgery. N Engl J Med. 2021 Nov 4. doi: 10.1056/NEJMoa2112299.
# Sabatine M, Bergmark B, Murphy S et al Percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting in left main coronary artery disease: an individual patient data meta-analysis Lancet. 2021 Dec 18;398(10318):2247-2257.
# Gaudino M, Hameed I, Di Franco A, Naik A, Demetres M, Biondi-Zoccai G, Bangalore S. Comparison of SYNTAX score strata effects of percutaneous and surgical revascularization trials: A meta-analysis J Thorac Cardiovasc Surg. 2021 Jun 2:S0022-5223(21)00881-3
# Piccolo R, Bonaa KH, Efthimiou O et al Drug-Eluting or Bare-Metal Stents for Left Anterior Descending or Left Main Coronary Artery Revascularization. Coronary Stent Trialists’ (CST) Collaboration. J Am Heart Assoc. 2021 Oct 19;10(20):e018828
# Correa-Sadouet C, Rodríguez-Granillo AM, Gallardo C et al; ORCA investigators. Randomized comparison between bare-metal stent plus colchicine versus drug-eluting stent alone in prevention of clinical adverse events after percutaneous coronary intervention. Protocol Future Cardiol. 2021 Jul;17(4):539-547
# Piccolo R, Bonaa KH, Efthimiou O, et al Drug-eluting or bare-metal stents for percutaneous coronary intervention: a systematic review and individual patient data meta-analysis of randomised clinical trials.Coronary Stent Trialists’ Collaboration.Lancet. 2019 Jun 22;393(10190):2503-25
# Zhang JJ, Ye F, Xu K, Kan J et al Multicentre, randomized comparison of two-stent and provisional stenting techniques in patients with complex coronary bifurcation lesions: the DEFINITION II trial. Eur Heart J. 2020 Jul 14;41(27):2523-2536
# Mieres J, Rodríguez AE, Fernández-Pereira C, Ascarrunz-Cattoretti D.Increased incidence of serious late adverse events with drug-eluting stents when compared with coronary artery bypass surgery: a cause of concern. Future Cardiol. 2020 Nov;16(6):711-723
# Valgimigli M, Campo G, Percoco et al; Multicentre Evaluation of Single High-Dose Bolus Tirofiban vs Abciximab With Sirolimus-Eluting Stent or Bare Metal Stent in Acute Myocardial Infarction Study (MULTISTRATEGY) Investigators.JAMA. 2008 Apr 16;299(15):1788-99
# Writing Committee Members, Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines J Am Coll Cardiol. 2021 Dec 7:S0735-1097(21)06157-X
# Deftereos SG, Beerkens FJ, Shah B et alColchicine in Cardiovascular Disease: In-Depth Review. Circulation. 2022 Jan 4;145(1):61-78. doi: 10.1161/CIRCULATIONAHA.121.056171.
# Matsumura-Nakano Y , Shiomi H, Morimoto T et alComparison of Outcomes of Percutaneous Coronary Intervention Versus Coronary Artery Bypass Grafting Among Patients With Three-Vessel Coronary Artery Disease in the New-Generation Drug-Eluting Stents Era (From CREDO-Kyoto PCI/CABG Registry Cohort-3) Am J Cardiol . 2021 Apr 15;145:25-36. doi: 10.1016/j.amjcard.2020.12.076.
# Toya T, Sara JD, Corban MT, Taher R et al Assessment of peripheral endothelial function predicts future risk of solid-tumor cancer Eur J Prev Cardiol. 2020 Apr;27(6):608-618.
# Abdul-Jawad Altisent,, Renier Goncalves-Ramírez L,Leticia Fernández et al Long-term Intra-coronary Structural and Vasomotor Assessment of the Absorb Bioresorbable Vascular Scaffold Am J of Cardiol Am J Cardiol. 2022 Jan 17;S0002-9149(21)01268-6. doi: 10.1016/j.amjcard.2021.12.037.
# Rajendran P, RengarajanT, Thangavel J et al The Vascular Endothelium and Human Diseases
International Journal of Biological Sciences 2013; 9(10):1057-1069
# Sidhu MS, Alexander KP, Huang Z et al Causes of Cardiovascular and Non-cardiovascular Mortality in the Ischemia Trial Originally published12 Nov 2020Circulation. 2020;142:A13030
# . Lopez-Sendon JL, Cyr DD, Mark DB et al Effects of initial invasive vs. initial conservative treatment strategies on recurrent and total cardiovascular events in the ISCHEMIA trial. Eur Heart J 2022;43:148–149.
# Rodriguez AE,Fernandez-Pereira C, Mieres J and A.Matias Rodriguez-Granillo Is non cardiac death increased with an initial invasive revascularization strategy? Commentary on the ISCHEMIA trial European Heart Journal Open (2022) 00, 1–2 https://doi.org/10.1093/ehjopen/oeac012
La Cardiología Intervencionista que viví en mis 41 años de práctica
I wish to thank the Argentine College of interventional Cardioangiologists (CACI) for giving me the extraordinary opportunity of becoming a founding member of the College and being able to practice this medical specialty for the past 40 years. .
In the following pages I will try to sum up what I think are the most important experiences lived by my colleagues and I since the beginning of this medical specialty including all that has been going on in this changing and fascinating specialty. Back in 1980, I was the Cardiology/Hemodynamics/Cardiovascular Surgery unit chief resident of Sanatorio Güemes, the then called Favaloro Foundation led by directors Dr. Rene G. Favaloro, and Dr. Luis de la Fuente at the time. It was then that we came up with our first tools to perform peripheral angioplasties of both femoral and renal arteries, still without the operative and technical capabilities to start this therapy in the coronary arteries.
Almost three years had gone by since Dr. Andreas Gruntzig had presented the first cases treated in Zurich, Switzerland back in 1977 in a meeting held by the American Heart Association.
Also, by then, in 1979, Dr, Peter Rentrop had already demonstrated the benefits of intracoronary thrombolysis with streptokinase for the reperfusion patients within the first few hours after an acute myocardial infarction.
Interventional cardiology as we know it was taking off.
It was precisely on October 3, 1980—my birthday by the way—that I had my first therapeutic experience using a catheter to treat the ischemic heart disease of a patient with an ST-segment elevation myocardial infarction.
The patient had sustained a 12-hour postoperative period following a side-to-side anastomosis of venous coronary artery bypass grafts to the left anterior descending coronary and diagonal arteries that showed signs of an extensive anterolateral infarction with hemodynamic compromise.
Dr. Favaloro called the cath lab. I talked to him and suggested the possibility of infusing thrombolytic drugs in the potential occlusion site, in other words, use the saphenous vein to perform the coronary artery bypass grafting.
The famous hematologist Dr. Raúl Altman, a collaborator of Dr. Favaloro, had urokinase available because he often used it for specific treatments.
With these elements we selectively catheterized the occluding bypass, proceeded with the 1-hour in-situ infusion of urokinase, and achieved the reperfusion of the diagonal artery and the entire proximal and middle third of the left anterior descending coronary artery resulting in TIMI grade-3 flow followed by complete hemodynamic stabilization.
I gladly remember Dr. Favaloro called me and told me: «Rodriguez this is the best birthday present you’re getting this year».
I presented the case at a South American congress of cardiology, and two years later it was published as a case report in the Journal of the American Heart Association with another case performed by a different member of the Hemodynamics staff unit.
Despite I personally performed this procedure skin to skin—as we say in our day-to-day medical jargon—I was deliberately excluded from the publication without my knowledge and while on one of my numerous trips to the United States during 1981 and 1982.
Back in 1980, Dr Richard Myler, an angioplasty pioneer in the United States, was giving lectures in Sanatorio Güemes as a guest of Dr. Favaloro. The opportunity was ripe for me to join his team, which I did in January 1981 for three months. Years later, Dr. Myler introduced and inducted me as a fellow of the American College of Cardiology.
At that time, I also had the opportunity of visiting Dr. John Simpson from Stanford University who was practicing with a new steerable system of catheters and moveable core metal guidewires to perform coronary angioplasties. Back in Argentina, in April, we started performing the first coronary angioplasties at Sanatorio Güemes.
Angioplasty in Europe and the United States was on the rise with pioneers like Dr. Andreas Gruntzig from Switzerland, and one of the most notorious of all, Dr. Geoffrey Hartzler from Kansas, United States who pioneered the field of myocardial infarction angioplasty. He is one of the greatest ever, there is no doubt about that. Dr. Hartzler was, unfortunately, gone before his time, but in 1982 he introduced the method to perform primary angioplasties without previous thrombolysis (a method called direct angioplasty).
At the time, acute myocardial infarction angioplasty was very controversial with conflicting results. Also, most angioplasties were being performed after the infusion of thrombolytic drugs.
At the end of 1981, one year after having performed the aforementioned intracoronary thrombolysis, I had the opportunity to perform an angioplasty after thrombolysis on a patient with an inferior wall ST-segment elevation myocardial infarction due to right coronary artery occlusion. The first thing I did was coronary artery reperfusion with the intracoronary infusion of urokinase and then perform the balloon angioplasty. The procedure was a success.
The case was published at the beginning of 1982 in the Argentine Journal of Cardiology. To my knowledge, this was the first case of coronary angioplasty after thrombolysis ever performed in Latin America in the acute myocardial infarction setting. Probably, only a German team had performed the same procedure that same year of 1982 publishing the case in Circulation.
During the 1980s our specialty skyrockets in the entire Western world both in the United States and Europe. Also, the late 1980s see the birth of plain old balloon angioplasty (POBA) and new devices like directional coronary atherectomy, rotablation, balloon dilatation catheters, and prolonged infusions, etc. allowing us to develop more complex angioplasties than the one initially performed by Dr. Gruentzig.
It wasn’t until the mid-1980s (1986) that we created our own clinical research working group, the Cardiovascular Research Center (CECI) based on Buenos Aires, Argentina. A research center that still stands today.
At that time, the first limited but very promising experiences with bare metal stents (BMS) to prevent coronary occlusions during balloon angioplasty were beginning to take shape. Names like Dr. Sigwart, Dr. Puel, Dr. Marco, Dr. Serruys, Dr. Roubin, and Dr. Palmaz started to make a difference in all scientific settings of our specialty.
# Decades of 1990/2000/2010. The dramatic ascent of coronary angioplasty as therapeutic procedure for the management of acute and chronic coronary patients.
In my humble opinion, these were the golden decades of our medical specialty.
The first decade of 1990/2000 witnessed a consolidation in the use of bare metal stents (BMS) during angioplasty to treat acute complications and coronary restenosis after POBA to avoid chronic and acute recoil after balloon angioplasty. At the time, this was the leading cause of restenosis after this procedure. The use of BMS was first introduced in the United States by Dr. Roubin and Dr. Palmaz with their balloon-expandable stents. Dr. Gianturco-Roubin’s was the first BMS approved by the FDA in the United States to treat acute complications followed shortly after by Palmaz-Schatz’s stents .
Stents eventually would be used in all clinical conditions including the acute myocardial infarction setting and very complex coronary lesions.
Also, this decade witnesses the publication of the first randomized clinical trials on coronary angioplasty with POBA vs coronary artery bypass graft (CABG) in patients with simple obstructions of multiple vessels, most of them with chronic coronary artery disease, also in diabetic patients. Shortly after these same comparisons would be made with the use of BMS . This is also the time when the first comparative randomized trials on acute myocardial infarctions treated with angioplasty vs thrombolysis are published followed by studies on angioplasty with POBA vs angioplasty with stenting .
During this decade two landmark meta-analyses confirmed that, in the long run, the angioplasty in patients with multivessel disease has the same survival and infarction-free survival rates compared to CABG excluding diabetic patients. In these analyses the survival rate of young patients showed a clear advantage towards the angioplasty, which is comprehensible, but was confirmed in this meta-analysis for the first time. The only difference in favor of CABG was the higher rate of new requirements for angioplasty revascularization.
Unfortunately, these findings were published,2008-2009, just when drug-eluting stents (DES) were on the rise, which is why these results were overlooked.
Although the use of bare metal stents minimized the occurrence of acute complications after angioplasty, it also caused in-stent restenosis due to fibrous intimal hyperplasia following the exaggerated scarring caused by new reinterventions of the target vessel within the first 8 to 10 months after stenting (> 20% rate).
The introduction of immunosuppressive drugs within the stent to be released in the arterial endothelium within the first month after stenting caused a significant reduction of this hyperplasia followed by a significant reduction of new revascularizations. Also, this combination prevented acute recoil and fibrous intimal hyperplasia.
This marked the beginning of DES that revolutionized our medical specialty. Actually, to this date, in certain discussion fora—not mine—they still revolutionize our specialty.
Esto es el inicio de los stents liberadores de fármacos (DES) que revolucionaron y aun hoy en algunos foros de discusión, no en el mío propio, siguen revolucionando nuestra especialidad. The names of Antonio Colombo, Eberhard Grube, Martin Leon, Patrick W. Serruys and Greg Stone are largely due to them this technological leap with the introduction of drug-eluting stents (DES). At this point, our colleague Eduardo Sousa and his group in Brazil also played an important role. However, our country was again not absent in this development of deS, and one of the observational studies in its use was carried out in Argentina by Dr Luis de la Fuente and despite the fact that his findings were not endorsed by a long multinational randomized European study, which had to be terminated prematurely due to excess of thrombotic complications of this DES design, this pilot study was pioneering at the time.
The significant reduction of new revascularizations reported after DES implantation brought expectations that were a little too optimistic regarding the use of stents like this. Rumor had it that «the end of restenosis would also be the end of CABG» following the early findings from the first randomized clinical trials on the use of DES. In the following section we will see how far we still are from these predictions.
This overoptimistic approach was built on reducing completely secondary and non-clinical endpoints to a minimum like minimizing the so-called “late loss” that could never be associated with the occurrence of hard endpoints after angioplasty.
# Decade of 2010/2021. The dramatic ascent of the indication of revascularization to the present day.
At this point I want to be very straightforward, but also very critical, and my opinions should also be taken from this personal point of view.
With the arrival of DES into the routine clinical practice, to this date, several randomized clinical trials including comparison groups have been conducted on angioplasty with DES vs CABG. As a matter of fact, up to 3 studies on unprotected left main coronary artery disease, 1 on multiple vessels and left main coronary artery, and the remaining 4 on multiple vessels including diabetic patients have been conducted.
From the beginning, all trials but 1 invariably showed more revascularization procedures as a natural companion of the angioplasty, which should not worry us. However, in 7 of these trials, the mortality and/or spontaneous myocardial infarction rates also went up, which is more disturbing and is associated with mortality.
The greater complexity of the patients treated could explain these findings, but it is probably not the only hypothesis. As a matter of fact, several meta-analyses proved that regardless of the anatomical complexity, the rate of hard endpoints like myocardial infarction—and in some studies, mortality—was lower with CABG.
This change in safety parameters in comparative studies with surgery had already been observed in the long American registry of ASCERT with 190 thousand patients treated with CABG and PCI (78% DES1) during the years 2004 to 2008 in 64 sites in the USA and where in patients >64 years there was a significant reduction in mortality with CABG even in groups of low angiographic and clinical risk (non-diabetic and two-vessel injury). and what a reason why we wrote a review article in 2012, where we already drew attention to these findings. This reference is among the suggested articles to read.
Although it is completely true that DES reduced significantly the rate of new revascularizations, mortality did not change when the old DES and/or even BMS designs were compared to the new ones.
With the first designs, the use of DES had 4 limitations some of which overlap:
1- Early, late, and very late stent thrombosis.
2- Poor late DES apposition. These 2 overlapped most of the times.
3- Early neo-atherosclerosis immediately after implantation (beyond 1st year).
4- Endothelial dysfunction both in the stent and in the proximal and distal segments of the implant.
Stent thrombosis and poor stent apposition were significantly associated with the polymer, but, to this date, this is not a problem anymore.
However, the 2 remaining ones—early neo-atherosclerosis and endothelial dysfunction—were mainly associated with the local action of the immunosuppressant drug. The former causes spontaneous infarctions not associated with new procedures that we have been invariably seeing in all randomized trials including comparison groups on CABG. Endothelial dysfunction is also associated with cardiac adverse events, but ultimately with non-cardiac adverse events too including a higher incidence rate of solid tumors.
It should not be forgotten that the endothelium is an organ with multiple functions such as: «vasodilation, thrombolysis, platelet disagreggation, antioxidant, antiinflammation, antiproliferation». The loss of its normal function i.e. endothelial dysfunction could produce the opposite effects: «vasocontriction, thrombosis, platelet agreggation, oxidant activity, inflammation and growth factors». At this point it is very important that interventional cardiologists define cost/benefit between suppression of restenosis / endothelial dysfunction and the clinical implications of the last one.
On this topic I recommend reading the manuscripts referenced below by Toya et al. and Abdul-Jawad Altisent et al., within the last references in this chapter.
It is surprising to see several observations associated with non-cardiac mortality in patients treated with angioplasty at the present time who were not in previous observations. Actually, this should be a cause for careful analysis in properly conducted randomized clinical trials and prospective registries. This increased non-cardiac mortality was reported not only in randomized clinical trials on DES and CABG, but also in comparisons of different DES designs. As we already know, large enough randomized clinical trials have the power to homogenize populations at a baseline level, which is why the explanation to this increased mortality should be looked for in other clinical settings. I recommend reading Gaudino’s meta-analysis, the 5 years of EXCEL trial, Pilgrim’s et al 5-year study of an «ultrathin DES», the CREDO-Kyoto registry of angioplasties and CABG all referenced below as well as the abstract of the ISCHEMIA trial published in Circulation in November of last year and the European Heart Journal this year. The publication of the last one was the reason of an Editorial comment of ours that is published in the European Heart Journal Open in February of this year and where in a Table we describe all the studies that reported an increase in non-cardiac death with DES in long-term follow-up, to these we must include the findings of the ISCHEMIA study that is really very worrying.
In my opinion calling non-cardiac mortality an adverse event due to coincidence is reckless, illogical, and eventually hurts our own medical specialty.
Only after a sincere discussion of all these findings with opinion leaders and industry CEOs we will be able to escape this labyrinth we fall into with every new randomized trial on CABG or with every medical therapy that only brings us frustration.
Lately even the introduction of methods of functional diagnosis of coronary lesions such as FFR or iFR to guide PCI have not been successful in demonstrating reduction of post-implantation events of DES both in patients with acute infarction or elective patients. I recommend reading the results published this year of randomized studies in this regard including FUTURE, FAME 3 and that of Puymirat E et al in acute myocardial infarction all referenced below between the suggested readings. The negative results of these studies with FFR show us that quickly interventional cardiologists adopt techniques and new «devices» often generating false expectations due to a hasty overestimation of the benefits.
Although the recently published new clinical guidelines on therapeutics elaborated together with clinical cardiologists are somehow benevolent to our medical specialty, they show that, unlike we thought 15 years ago, despite the arrival of state-of-the-art DES designs, coronary artery bypass grafting is more alive than ever. In fact, both American (USA) and European Societies of Cardiovascular and Thoracic surgery didn’t endorse that guideline.
# Creation of the Cardiovascular Research Center (CECI).
In 1986 together with colleagues and friends we formed an independent working group first in the Anchorena Sanatorium and then moved to the Otamendi Sanatorium from 1993 to the present.
During all these years there are no words to describe the support for all our care and scientific tasks developed in the Otamendi, so my thanks to your past authorities Drs. Jose A. De All for whoever comes to work in this Institution and Dr Jorge Aufiero as well as the current authorities.
During all these years, many cardiologists went through the Service to be trained in the practice of our specialty, many of them today Heads of Service in reference places in our country as well as prominent members of scientific societies that could not list them by the quantity, both in our country and in Latin America. Residents of almost all nationalities of the Spanish- and Portuguese-speaking region passed through the service from Paraguay, Chile, Brazil, Bolivia, Peru, Uruguay, Ecuador, Venezuela, Colombia, Panama and the Dominican Republic who then continued to be connected with us, often carrying out joint research work.
Back in 1988, two years after creating a working group with friends and colleagues, we teamed up again to create an independent department of clinical research. Although it was not created as a CRO (there are several examples of excellent CROs in Argentina), it allowed us to arrange multiple research protocols in our country in an orderly fashion, and one by one at the beginning. Afterwards, we conducted multicenter studies including international clinical trials.
Here is a summary of the most significant clinical trials conducted that I think played a key role in our routine clinical practice:
This whole thing started with the first randomized clinical trial published on coronary angioplasty with POBA vs CABG—the ERACI I trial—published in JACC in 1993 and 1995. Years later with the arrival of BMS, the second version of this study, the ERACI II, was published. Unlike the ERACI I, this multicenter trial was co-authored by the fondly remembered Dr. Liliana Grinfeld. Both manuscripts were published in JACC in 2001 and 2005 including the 1- and 5-year follow-up simultaneously published with Dr. Patrick Serruys’ ARTS study.
Back in 1993, we published an observation suggesting that restenosis after balloon angioplasty was mainly due to acute artery recoil after balloon dilatation. Something completely new that we had never associated. In the animal model of restenosis common knowledge was that the endothelial damage due to the mechanism of the angioplasty triggered vessel restenosis months later. However, this was not the case with human beings in whom atherosclerotic plaque is often eccentric and behaves different from the balloon in such a way that the rate of restenosis was very low in lesions whose diameter did not change 24 hours after balloon angioplasty. This finding was published in several scientific journals: American Journal of Cardiology in 1993 and 1995, Circulation in 1995, and JACC in 1998 and also of academic discussions with world opinion leaders since they spoke of: «.. coronary restenosis a time related phenomenom…» therefore our observations were totally opposite and were the subject of controversy. Time proved us right and Patrick Serruys ended up accepting that acute recoil was a very important phenomenon in the pathophysiology of post POBA restenosis, there he began talking about «stent like results post POBA» in other words optimal post-balloon results without acute recoil.
It was very pleasant 3 years ago to see in the gallery of the PCR Congress exposed as one of the milestones of angioplasty precisely the work of our stent in elastic recoil OCBAS trial that was published in JACC 1998 together with the ERACI I and II studies.
In the same sense, it was also very pleasant to read in the book on the history of cardiovascular interventions and interventional cardiology that one of its greatest pioneers Gary Roubin whose aforementioned book was entitled «The First Balloon-Expandable Coronary Stent an Expedition That Changed Cardiovascular Medicine» published in 2015 included us along with Julio Palmaz and Rene Favaloro as the only Latin Americans in the list of the 93 pioneers of Angioplasty and Cardiovascular Interventions, this reference is also within the suggested lectures of this chapter.
The use of stent in the acute myocardial infarction setting is appealing but was also very controversial too. Together with the beloved Dr. Gary Roubin our group published a short experience on the use of stent in the ST-segment elevation myocardial infarction setting in the American Journal of Cardiology back in 1996. This experience immediately turned into the first study on the use of stents in the acute myocardial infarction setting accepted for publication. The GRAMI trial—published in the American Journal of Cardiology in 1998—was contemporaneous to Dr. David Antoniucci’s study. Actually, his study was published two months prior to the JACC publication, but ours had already been accepted two months before the Florence study. Therefore, both chronologically and academically we came first. Anecdotes I always like to remember in our family reunions with my great Italian friend.
Already in the new millennium, the CECI Center participated in prospective records and observational studies such as those related to DES thrombosis published in EuroIntervention in February 2007 («Late stent thrombosis the Damocles sword of DES») a month before the promoted article by Camenzid and Wijns in Circulation, the ERACI III record, which was published in JACC in 2006 and in the Eur Heart J in 2007 this last work was one of the reason why this European Journal will increase its «impact factor» according to a personal letter we received from the Editor-in-Chief of that Journal.
The review article on «DES late thrombosis» there were friends who recommended me not to publish it because it could have adverse reactions from the industry that manufactured the DES, despite those tips, the work was sent and then review accepted and published in EuroIntervention. I must also say that I never felt an adverse reaction from the industry for this.
If the doctors of the CACI specialty career wonder how we were able from Argentina to carry out so many studies that were published in the largest English-speaking «Journals» I would tell them that everything is achieved with work and a lot of honesty in the analysis and observation of the facts that one is seeing. You should always be sure of what you are saying, and you should always check the information several times before making a further judgment if this implies original findings outside of what is established and expected. In fact, at the time where these thoughts were writing, April 30 th, 2022, according Research Gate scientific data manuscripts published by us as authors or coauthors deserved 26222 reads,7568 citations and have 3920 points of research interest the largest numbers achieve by any group or individual person in our country in the area of interventional cardiology.
Controversies with our findings happened in several times, with the «elastic recoil», the ERACI studies and with stent in acute myocardial infarction. In these points the collaboration with Igor Palacios, Gary Roubin, John Ambrose, William O’Neill and David Antoniucci were very important. As I said on the occasion of a distinction granted to me by the Legislature of CABA: » the work we did here in Argentina with ideas totally ours and our patients, but nothing would have been the same if our friend from USA or EU didn’t support to us «.
In the ERACI I study, which Favaloro was very angry when we did and spoke ill of the findings including trying to convince the surgeon who had operated on almost all patients not to sign the manuscript once it was approved in the JACC, an Argentine work published in the JACC in 1993 had few precedents in the cardiology of our country, finally cousin rationality and the surgeon signed the work, Dr Néstor Perez-Balino was a faithful witness of what I am recounting. I had, however, the pleasure that several years later, in May 2000, when the new ERACI II had already been accepted for publication, Favaloro called me by phone to congratulate me personally on this work and with warm memories of the past shared in a very difficult moment of the Foundation and also personal of him few months before his death.
Over the last 20 years, the Cardiovascular Research Center (CECI) has conducted several multinational and randomized clinical trials on several DES designs and different revascularization strategies in patients with acute myocardial infarction, as well as in chronic patients.
In this way we participate in the abciximab in acute infarction with a carbon metal stent, JESTENT rheolithic thrombectomy in acute infarction, FREEDOM, FREEDOM long term outcome DES vs CABG in diabetic patients, MULTISTRATEGY on DES and abciximab in acute infarction, VALENTINES with Paclitaxel releasing balloon, DEFINITION II treatment of bifurcations with DES including lesions of unprotected trunk and lately MASTER DAPT comparison of antiplatelet strategy with DES, all of them published several times in NEJM, JAMA, JACC, Circulation, Eur Heart Journal, JACC Intervention and EuroIntervention
Similarly, our database was submitted for analysis and control through several meta-analyses, and eventually, the ERACI and ERACI II clinical trials were submitted for publication (Dr. Pocok in The Lancet, 1995; Dr. Hlatky in The Lancet, 2009 and JACC in 2012; Dr. Daemen in Circulation, 2008, and Dr. Head in The Lancet back in 2018).
Likewise, the database of the EUCATAX trial was submitted to Dr. Valgimigli for the publication of his meta-analysis in The Lancet in 2019, and Circulation in 2021.
Also, based on a prospective registry of multiple vessels, is that the ERACI Score was born as a revascularization strategy in patients with multi-vessel disease and left coronary trunk, which was a joint product of several centers in our country and that tries to reduce the number of DES implanted following anatomical schemes of vessel size and degree of stenosis by angiography, this Score was validated with both the use of DES and BMS.
Last but not least, the studies on the systemic prevention of restenosis with oral immunosuppressant and anti-inflammatory agents after BMS implantation.
Although in the era of balloon angioplasty this strategy did not had favorable results—as a matter of fact no positive results could come from it because the pathophysiology was not inflammatory—in the era of bare metal stents all the randomized clinical trials conducted by us and European working groups in Germany, Italy, Serbia, and Greece on immunosuppressant drugs like rapamycin and/or prednisone had positive results that were summed up in a meta-analysis published by Dr. Kastrati in 2014. Still this strategy was never part of the routine clinical practice.
At this moment, we are conducting a cost-effective randomized clinical trial between state-of-the-art DES vs BMS plus a 3-month course of colchicine only in the BMS group that is still in the recruiting phase. We can only hope it will be completed in the next months.
Given the conflicting and somehow unexpected long-term results with DES, I still believe all options should be on the table and none should be discarded to achieve a greater mid- and long-term efficacy and safety with our percutaneous revascularization procedures whether coronary angioplasty with DES implantation in bifurcation lesions probably including most of unprotected left main coronary artery disease, and BMS implantation in more favorable anatomies, and/or a combination of both strategies.
Nothing should be left out if we want our patients to benefit the most, and if we want to improve this medical specialty that has shaped our lives for so long.
In the last Editor Letter we wrote at JAMA at the beginning of 2021 we told the Editor-in-Chief of the Journal that we thought it was important to publish our letter because we felt that: ….»coronary angioplasty is on the cross roads«…
We need to honestly explain and discuss the origin of our failures and redefine the technique, the «devices» and the indications in another way only the current and new generations of interventional cardiologists will have the niches of patients with acute infarction in progress and / or terminal patients with contraindication of CABG or very short life expectance.
Very little for such a rich history!!!
References suggested
#-Gruentzig AR, Senning A, Siegenthaler WE. Nonoperative dilation of coronary
artery stenosis. Percutaneous transluminal coronary angioplasty.N Eng J Med 1979;301:61-8.
#-Rentrop KP, Cohen M, Hosat ST. Thrombolytic therapy in acute myocardial infarction: review of clinical trials. Am J Cardiol. 1984 Dec 21;54(11):29E-31E
#–Hartzler GO, Rutherford BD, McConahay DR et al: Percutaneous translu-minal coronary angioplasty with and without thrombolytic therapy for treatment of acute myocardial infarction. Am Heart J 1983; 106:965–973.
#- Rodríguez AE, Diaz R, Zuffardi E, Navarro P, de la Fuente LM. Angioplastia
transluminal percutánea coronaria. Rev Arg Cardiol 1982;50(2):78-91.
#. Sigwart U, Puel J, Mirkovich V, Joffre E, Kappenberger L. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty.N Eng J Med 1987;316:701-6.
#. Serruys PW, Juilliere Y, Bertrand ME, Puel J, Rickards AF, Sigwart U. Additionalimprovement of stenosis geometry in human coronary arteries by stenting after balloon dilatation. Am J Cardiol 1988 May9;61(14):71G-76G.
#. Roubin G, Gianturco C, Brown J, Robinson K, King S. Intracoronary stenting of canine coronary arteries after percutaneous coronary angioplasty. Circulation 1986;1986:74.
#. Palmaz JC, Windeler SA, Garcia F, et al. Atherosclerotic rabbit aortas: expandable intraluminal grafts. Radiology 1986;160:723-6.
# Palmaz JC. Balloon expandable intravascular stent. Am J Roentgenol 1988;150,1263-9.
#. Roubin G, Douglas JR, Lembo NJ, Black AJ, King S. Intracoronary stenting for acute closure following percutaneous coronary angioplasty. Circulation 1988;78:407.
#. Schatz RA, Baim DS, Leon M, et al. Clinical experience with the Palmaz-Schatz coronary stent. Initial result of a multicenter study. Circulation 1991;83:148-61.
#. Roubin G, Cannon AD, Agrawal SK, et al. Intracoronary stenting for acuteand threatened closure complications after transluminal coronary angioplasty. Circulation 1992; 85:916-27.
#. Sousa JE, Costa MA, Abizaid AC, et al. Sustained suppression of neointimal proliferation by sirolimus-eluting stents: one-year angiographic and intravascularultrasound follow-up. Circulation 2001 Oct 23;104(17):2007-11.
#. Rensing BJ, Vos J, Smits PC, et al. Coronary restenosis elimination with a sirolimus eluting stent: first European human experience with 6-month angiographic and intravascular ultrasonic follow-up. Eur Heart J 2001;22(22):2125-30
#Serruys PW, Degertekin M, Tanabe K, et al. RAVEL Study Group. Intravascularultrasound findings in the multicenter, randomized, double-blind RAVEL (RAndomized study with the sirolimus-eluting VElocity balloon-expandable stent in the treatment of patients with de novo native coronary artery Lesions) trial. Circulation 2002 Aug 13;106(7):798-803.
#. Grube E, Silber S, Hauptmann KE, et al. TAXUS I: six- and twelve-month results from a randomized, double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesions. Circulation 2003 Jan 7;107(1):38-42.
#. Colombo A, Drzewiecki J, Banning A, et al. TAXUS II Study Group. Randomized study to assess the effectiveness of slow- and moderate-release polymer-based paclitaxel-eluting stents for coronary artery lesions. Circulation 2003 Aug 19;108(7):788-94.
# de la Fuente LM, Miano J, Mrad J et al. Initial results of the Quanam drug eluting stent (QuaDS-QP-2) Registry (BARDDS) in human subjects. Catheter Cardiovasc Interv 2001;53(4):480-8.
#. Grube E, Lansky A, Hauptmann KE, et al. SCORE randomized trial. High-dose 7-hexanoyltaxol-eluting stent with polymer sleeves for coronary revascularization: one-year results from the SCORE randomized trial. J Am Coll Cardiol 2004 Oct 6;44(7):1368-72.
# Rodríguez AE, Santaera O, Larribau M, Sosa MI, Palacios IF. Early decrease in minimal luminal diameter after successful percutaneous transluminal coronary angioplasty predicts late restenosis. Am J Cardiol 1993;71: 1391-5.
#. Rodríguez AE, Santaera O, Larribau M et al. Coronary stenting decreases restenosis in lesions with early loss in luminal diameter 24 hours after successful PTCA. Circulation 1995;91:1397-402.
# Rodríguez A, Ayala F, Bernardi V, Santaera O, Marchand E, Pardiñas C, Mauvecin C, Vogel D, Harrell LC, Palacios IF. Optimal coronary balloon angioplasty with provisional stenting versus primary stent (OCBAS): immediate and long-term follow-up results. J Am Coll Cardiol 1998 Nov;32(5):1351-7.
#. Fischman DL, Leon MB, Baim D, et al. A randomized comparison of coronary stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501.
# Serruys PW, de Jaegere P, Kiemeneij F et al, for the BenestentStudy Group. A comparison of balloon expandable stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-95.
#. * Rodríguez A, Boullon F, Pérez Baliño N, Paviotti C, Sosa Liprandi MI, Palacios IF. Argentine Randomized Trial of Percutaneous Transluminal Coronary Angioplasty Versus Coronary Artery Bypass Surgery in Multivessel Disease (ERACI): in-hospital results and 1-year follow-up. J Am Coll Cardiol 1993;22:1060-7.
#. Hampton JR, Handerson RA, Julian DG, et al. Coronary angioplasty versus coronary artery bypass surgery: the Randomized Intervention Treatment of Angina (RITA) trial. Lancet 1993;343:573-80.
#. King SB III, Lembo NJ, Weintraub WS, et al., for the Emory Angioplasty Surgery Trial (EAST). A randomized trial comparing coronary angioplasty with coronary artery bypass surgery. N Engl J Med 1994;331:1044-50.
#. Hamm CW, Reimers J, Ischinger T, Rupprecht HJ, Berger J, Bleifeld W, for the German Angioplasty Bypass Surgery Investigation. A randomized study of coronary angioplasty compared with bypass surgery in patients with symptomaticm ultivessel coronary disease. N Engl J Med 1994;331:1037-43.
#. Rodríguez AE, Bernardi V, Navia J et al. Argentine Randomized Study: Coronary Angioplasty with Stenting versus Coronary Bypass Surgery in Patients with Multiple Vessel Disease (ERACI II): 30 days results and on year follow-up results. J Am Coll Cardiol 2001;3:51-8.
#. Serruys PW, Unger F. Sousa JE, et al. Comparison of coronary artery bypass surgery and stenting for the treatment of multi-vessel disease. N Engl J Med 2001;344:1117-24.
#. SoS Investigators Coronary Artery Bypass Surgery versus percutaneous coronary intervention with stent implantation in patients with multi-vessel coronary artery disease (the Stent or Surgery trial): a randomized controlled trial. Lancet 2002;360:965-70.
#. Hueb W, Soares P, Gersh B, et al. The Medicine, Angioplasty, or Surgery Study (MASS II trial): a randomized controlled clinical trial of three therapeutic strategies for multi-vessel coronary artery disease. J Am Coll Cardiol 2004;43:1743-51.
#Roubin GS The First Balloon Expandable Coronary Stent, An Expedition that change Cardiovascular Medicine: A Memoir. University of Queensland Press, St Lucia Queesnland, Australia 2014
#. Grines CL, Cox DA, Stone GW, et al. Coronary angioplasty with or without stent implantation for acute myocardial infarction. N Engl J Med 1999; 341:1949-56.
#. Rodríguez AE, Fernández M, Santaera O et al. Coronary stenting in patients undergoing percutaneous transluminal coronary angioplasty during acute myocardial infarction. Am J Cardiol 1996 Apr 1;77(9):685-9.
#. Rodríguez AE, Bernardi V, Fernández J et al. In-hospital and late results of coronary stents versus conventional balloon angioplasty in acute myocardial infarction (GRAMI trial). Gianturco- Roubin in Acute Myocardial Infarction. Am J Cardiol 1998 Jun 1;81(11):1286-91.
#- Antoniucci D, G.M. Santoro, L. Bolognese, R. Valenti, M. Trapani, P.F. Fazzini A clinical trial comparing primary stenting of the infarct-related artery with optimal primary angioplasty for acute myocardial infarction J Am Coll Cardiol, 31 (1998), pp. 1234-1239
#. Cassese S, De Luca G, Ribichini F et al. ORAl iMmunosuppressivether apy to prevent in-Stent rEstenosiS (RAMSES) cooperation: a patient-level meta-analysis of randomized trials. Atherosclerosis 2014 Dec;237(2):410-7.
#. Hlatky MA, Boothroyd DB, Bravata DM et al.Coronary artery bypass surgery compared with percutaneous coronary interventions for multivessel disease: a collaborative analysis of individual patient data from ten randomised trials. Lancet 2009 Apr 4;373(9670):1190-7.
#. Rodríguez AE, Mieres J, Fernández-Pereira C et al. Coronary stent thrombosis in thecurrent drug-eluting stent era: insights from the ERACI III trial. J Am Coll Cardiol 2006 Jan 3;47(1):205-7. Epub 2005 Dec 9.
#. Rodríguez AE, Rodríguez-Granillo GA, Palacios IF. Late stent thrombosis the Damocles sword of Drug Eluting Stents. Eurointervention 2007 Feb; 2(4) 512-7.
#. Camenzind E, Steg PG, Wijns W. Stent thrombosis late after implantation of first-generation drug-eluting stents: a cause for concern. Circulation 2007 Mar 20;115(11):1440-55; Epub 2007 Mar 7.
# Rodríguez AE, Maree AO, Mieres J et al.Late loss of early benefit from drug eluting stents when compared with bare metal stents and coronary artery bypass surgery: 3 years follow up of ERACI III registry. Eur Heart J 2007 Sep;29 (17):2118-25.
# Rodríguez AE, Fernández-Pereira C, Rodríguez-Granillo AM.Changes in the safety paradigm with percutaneous coronary interventions in the modern era: Lessons learned from the ASCERT registry.World J Cardiol. 2012 Aug 26;4(8):242-9. doi: 10.4330/wjc.v4.i8.242.
#. Dangas GD, Farkouh ME, Sleeper LA et al, FREEDOM Investigators. Long-term outcome of PCI versus CABG in insulin and non-insulin-treated diabetic patients: results from the FREEDOM trial. J Am Coll Cardiol 2014 Sep 23;64(12):1189-97.
#. Antoniucci D, Rodríguez AE, Hempel A et al, A randomized trial comparing primary infarct artery stenting with or without abciximab in acute myocardial infarction. J Am Coll Cardiol 2003 Dec 3;42(11):1879-85.
# Waksman R, Serra A, Loh JP et al. Drug-coated balloons for de novo coronary lesions: results from the Valentines II trial. EuroIntervention 2013 Sep;9(5):613-9.
# Rodríguez AE, Vigo CF, Delacasa A et al,; EUCATAX Investigators. Efficacy and safety of a double-coated paclitaxel-eluting coronary stent: the EUCATAX trial. Catheter Cardiovasc Interv 2011Feb 15;77(3):335-42.
# Zhang JJ, Ye F, Xu K, Kan J, Tao L et al Multicentre, randomized comparison of two-stent and provisional stenting techniques in patients with complex coronary bifurcation lesions: the DEFINITION II trial. Eur Heart J. 2020 Jul 14;41(27):2523-2536
# Rodriguez AE, Fernandez-Pereira C, Mieres J, Santaera O, Antoniucci D; ERACI IV investigators. Modifying angiographic syntax score according to PCI strategy: lessons learnt from ERACI IV Study.Cardiovasc Revasc Med. 2015 Oct-Nov;16(7):418-20. doi: 10.1016/j.carrev.2015.07.001
# Rodriguez AE, Fernandez-Pereira C, Mieres J, et al Lowering risk score profile during PCI in multiple vessel disease is associated with low adverse events: The ERACI risk score.Cardiovasc Revasc Med. 2018 Oct;19(7 Pt A):792-794
# Rioufol G, Dérimay F, Roubille F,et al Fractional Flow Reserve to Guide Treatment of Patients With Multivessel Coronary Artery Disease.FUTURE Trial Investigators.J Am Coll Cardiol. 2021 Nov 9;78(19):1875-1885
# Fearon WF, Zimmermann FM, De Bruyne B et al Fractional Flow Reserve-Guided PCI as Compared with Coronary Bypass SurgeryN Engl J Med . 2021 Nov 4. doi: 10.1056/NEJMoa2112299. Online ahead of print.
# Puymirat E, Cayla G, Simon T et al Multivessel PCI Guided by FFR or Angiography for Myocardial Infarction N Engl J Med. 2021 Jul 22;385(4):297-308.,
# Gaudino, M; Hameed, I; Farkouh ME et al, Overall and Cause-Specific Mortality in Randomized Clinical Trials Comparing Percutaneous Interventions With Coronary Bypass Surgery A Meta-analysis; JAMA Intern Med. doi:10.1001/jamainternmed.2020.4748 Published online October 12, 2020.
# Rodríguez-Granillo AM, Fernández-Pereira C, Rodríguez AE.Drug-Eluting vs Bare-Metal Stents for Percutaneous Coronary Intervention. JAMA Intern Med. 2021 Jul 1;181(7):1012-1013. doi: 10.1001/jamainternmed.2021.0030.
# Head SJ, Milojevic M, Daemen J, et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet 2018;391:939–48.
# Stone GW, Kappetein AP, Sabik JF et al Five-Year Outcomes after PCI or CABG for Left Main Coronary Disease.EXCEL Trial Investigators. N Engl J Med. 2019 Nov 7;381(19):1820-1830
# Park DW, Ahn JM, Yun SC, et al. Ten-year outcomes of stents versus coronary artery bypass grafting for left main coronary artery disease. J Am Coll Cardiol 2018;72 Pt A:2813–22.
# Pavlovsky H, Rodriguez-Granillo AM, Rodriguez AE.Late Mortality After Drug-Eluting, Bare-Metal Stents, and Coronary Bypass Surgery in Left Main Disease. J Am Coll Cardiol. 2019 Apr 9;73(13):1737
# Holm NR, Mäkikallio T, Lindsay MM et al NOBLE investigators. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet. 2020 Jan 18;395(10219):191-
# Daemen J, Boersma E, Flather M et al Long-term safety and efficacy of percutaneous coronary intervention with stenting and coronary artery bypass surgery for multivessel coronary artery disease: a meta-analysis with 5-year patient-level data from the ARTS, ERACI-II, MASS-II, and SoS trials. Circulation. 2008 Sep 9;118(11):1146-54.
# Flather M, Rhee JW, Boothroyd DB et al The effect of age on outcomes of coronary artery bypass surgery compared with balloon angioplasty or bare-metal stent implantation among patients with multivessel coronary disease. A collaborative analysis of individual patient data from 10 randomized trials.J Am Coll Cardiol. 2012 Nov 20;60(21):2150-7.
# Pilgrim T, Piccolo R, Heg D et al Ultrathin-strut, biodegradable-polymer, sirolimus-eluting stents versus thin-strut, durable-polymer, everolimus-eluting stents for percutaneous coronary revascularisation: 5-year outcomes of the BIOSCIENCE randomised trial Lancet. 2018 Sep 1;392(10149):737-746.
# Hironori H, Masafumi On, Hideyuki K, et al Impact of stent length and diameter on 10-year mortality in the SYNTAXES trial Catheter Cardiovasc Interv . 2021 Sep;98(3):E379-E387.
# Gomes WJ, Albuquerque LC, Jatene FB, Leal JCF, Rocha EAV, Almeida RMS.The transfiguration of the EXCEL trial: exceeding ethical and moral boundaries.Eur J Cardiothorac Surg. 2020 Jul 1;58(1):30-34.
# Fearon WF, Zimmermann FM, De Bruyne B et al; FAME 3 Investigators.Fractional Flow Reserve-Guided PCI as Compared with Coronary Bypass Surgery. N Engl J Med. 2021 Nov 4. doi: 10.1056/NEJMoa2112299.
# Sabatine M, Bergmark B, Murphy S et al Percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting in left main coronary artery disease: an individual patient data meta-analysis Lancet. 2021 Dec 18;398(10318):2247-2257.
# Gaudino M, Hameed I, Di Franco A, Naik A, Demetres M, Biondi-Zoccai G, Bangalore S. Comparison of SYNTAX score strata effects of percutaneous and surgical revascularization trials: A meta-analysis J Thorac Cardiovasc Surg. 2021 Jun 2:S0022-5223(21)00881-3
# Piccolo R, Bonaa KH, Efthimiou O et al Drug-Eluting or Bare-Metal Stents for Left Anterior Descending or Left Main Coronary Artery Revascularization. Coronary Stent Trialists’ (CST) Collaboration. J Am Heart Assoc. 2021 Oct 19;10(20):e018828
# Correa-Sadouet C, Rodríguez-Granillo AM, Gallardo C et al; ORCA investigators. Randomized comparison between bare-metal stent plus colchicine versus drug-eluting stent alone in prevention of clinical adverse events after percutaneous coronary intervention. Protocol Future Cardiol. 2021 Jul;17(4):539-547
# Piccolo R, Bonaa KH, Efthimiou O, et al Drug-eluting or bare-metal stents for percutaneous coronary intervention: a systematic review and individual patient data meta-analysis of randomised clinical trials.Coronary Stent Trialists’ Collaboration.Lancet. 2019 Jun 22;393(10190):2503-25
# Zhang JJ, Ye F, Xu K, Kan J et al Multicentre, randomized comparison of two-stent and provisional stenting techniques in patients with complex coronary bifurcation lesions: the DEFINITION II trial. Eur Heart J. 2020 Jul 14;41(27):2523-2536
# Mieres J, Rodríguez AE, Fernández-Pereira C, Ascarrunz-Cattoretti D.Increased incidence of serious late adverse events with drug-eluting stents when compared with coronary artery bypass surgery: a cause of concern. Future Cardiol. 2020 Nov;16(6):711-723
# Valgimigli M, Campo G, Percoco et al; Multicentre Evaluation of Single High-Dose Bolus Tirofiban vs Abciximab With Sirolimus-Eluting Stent or Bare Metal Stent in Acute Myocardial Infarction Study (MULTISTRATEGY) Investigators.JAMA. 2008 Apr 16;299(15):1788-99
# Writing Committee Members, Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines J Am Coll Cardiol. 2021 Dec 7:S0735-1097(21)06157-X
# Deftereos SG, Beerkens FJ, Shah B et alColchicine in Cardiovascular Disease: In-Depth Review. Circulation. 2022 Jan 4;145(1):61-78. doi: 10.1161/CIRCULATIONAHA.121.056171.
# Matsumura-Nakano Y , Shiomi H, Morimoto T et alComparison of Outcomes of Percutaneous Coronary Intervention Versus Coronary Artery Bypass Grafting Among Patients With Three-Vessel Coronary Artery Disease in the New-Generation Drug-Eluting Stents Era (From CREDO-Kyoto PCI/CABG Registry Cohort-3) Am J Cardiol . 2021 Apr 15;145:25-36. doi: 10.1016/j.amjcard.2020.12.076.
# Toya T, Sara JD, Corban MT, Taher R et al Assessment of peripheral endothelial function predicts future risk of solid-tumor cancer Eur J Prev Cardiol. 2020 Apr;27(6):608-618.
# Abdul-Jawad Altisent,, Renier Goncalves-Ramírez L,Leticia Fernández et al Long-term Intra-coronary Structural and Vasomotor Assessment of the Absorb Bioresorbable Vascular Scaffold Am J of Cardiol Am J Cardiol. 2022 Jan 17;S0002-9149(21)01268-6. doi: 10.1016/j.amjcard.2021.12.037.
# Rajendran P, RengarajanT, Thangavel J et al The Vascular Endothelium and Human Diseases
International Journal of Biological Sciences 2013; 9(10):1057-1069
# Sidhu MS, Alexander KP, Huang Z et al Causes of Cardiovascular and Non-cardiovascular Mortality in the Ischemia Trial Originally published12 Nov 2020Circulation. 2020;142:A13030
# . Lopez-Sendon JL, Cyr DD, Mark DB et al Effects of initial invasive vs. initial conservative treatment strategies on recurrent and total cardiovascular events in the ISCHEMIA trial. Eur Heart J 2022;43:148–149.
# Rodriguez AE,Fernandez-Pereira C, Mieres J and A.Matias Rodriguez-Granillo Is non cardiac death increased with an initial invasive revascularization strategy? Commentary on the ISCHEMIA trial European Heart Journal Open (2022) 00, 1–2 https://doi.org/10.1093/ehjopen/oeac012
Read MoreEl 7 de Diciembre se realizó una nueva edición de nuestro prestigioso Simposio
Aqui podra verlo en forma completa
Indicaciones y resultados del cierre del foramen oval permeable
Estado actual de la antiagregación y anticoagulación en los síndromes coronarios agudos post angioplastia
Estado actual del tratamiento Percutáneo de las Válvulas Aórtica y Mitral
¿Revascularización miocárdica 2021 que nos dice la evidencia actual y pasada?

El próximo 17 de noviembre se realizará el Congreso anual del Centro de Estudios en Cardiología Intervencionista (CECI). Para verlo ingresar al siguiente link: https://videmecum.com/webinar-ceci/

Estudio recientemente publicado asignó aleatoriamente a los pacientes con estenosis aórtica grave y riesgo quirúrgico bajo a someterse a una TAVR con colocación transfemoral de una válvula expandible por balón o cirugía. El objetivo primario fue un compuesto de muerte, accidente cerebrovascular o rehospitalización a 1 año. Como resultado, entre los pacientes con estenosis aórtica grave que tenían un riesgo quirúrgico bajo, la tasa de muerte compuesta, accidente cerebrovascular o reingreso hospitalario a 1 año fue significativamente menor con la TAVR que con la cirugía.
Link: https://www.nejm.org/doi/full/10.1056/NEJMoa1814052
Read MoreLa finalidad del estudio fue evaluar los resultados clínicos y la hemodinamia de la válvula cardíaca transcatéter un año después de TAVR en pacientes de bajo riesgo. El objetivo primario fue mortalidad de cualquier causa a 30 días. Los objetivos secundarios incluían resultados clínicos y la hemodinamia valvular a 1 año. Como resultado, la TAVR en pacientes de bajo riesgo con estenosis aórtica severa sintomática parece ser segura al cabo de 1 año. El engrosamiento de la lámina hipoatenuada, observado en una minoría de pacientes con TAVR a 30 días, no afectó la hemodinamia de las válvulas a largo plazo.
Link: http://interventions.onlinejacc.org/content/early/2019/03/12/j.jcin.2019.03.002
Read More
Se publicó un estudio en el New England Journal of Medicine en el que se realizó un ensayo randomizado, comparándose TAVR con una bioprótesis supraanular autoexpandible con el reemplazo quirúrgico de la válvula aórtica en pacientes con estenosis aórtica grave y riesgo quirúrgico bajo. El objetivo primario fue un compuesto de muerte o accidente cerebrovascular incapacitante a los 24 meses, utilizando métodos Bayesianos. Como resultado, en pacientes con estenosis aórtica grave que tenían un riesgo quirúrgico bajo, la TAVR con una bioprótesis supraanular autoexpandible no fue inferior a la cirugía con respecto al objetivo compuesto de muerte o accidente cerebrovascular incapacitante a los 24 meses.
Link: https://www.nejm.org/doi/full/10.1056/NEJMoa1816885
Read MoreEn un estudio publicado en el JACC, el FREEDOM trial evaluó la supervivencia a largo plazo de pacientes diabéticos con enfermedad multivaso sometidos a revascularización coronaria. Se randomizaron a 1900 pacientes diabéticos con enfermedad multivaso que se sometieron a PCI, con stents liberadores de sirolimus o paclitaxel, o CABG. Como resultado, en los pacientes diabéticos y con enfermedad multivaso la revascularización coronaria con CABG conduce a una menor mortalidad por todas las causas que con PCI-DES en el seguimiento a largo plazo.
Link: http://www.onlinejacc.org/content/73/6/629
Read More